|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Optical coherence tomography angiographyСтр 1 из 4Следующая ⇒
Author Lakshmana M Kooragayala, MD
Specialty Editor Board Francisco Talavera, PharmD, PhD
Steve Charles, MD Chief Editor Douglas R Lazzaro, MD, FAAO, FACS Additional Contributors V Al Pakalnis, MD, PhD
https: //emedicine.medscape.com/article/1223746-overview#showall
Overview Background Central retinal vein occlusion (CRVO) is a common retinal vascular disorder. Clinically, CRVO presents with variable visual loss; the fundus may show retinal hemorrhages, dilated tortuous retinal veins, cotton-wool spots, macular edema, and optic disc edema. Note the images below.
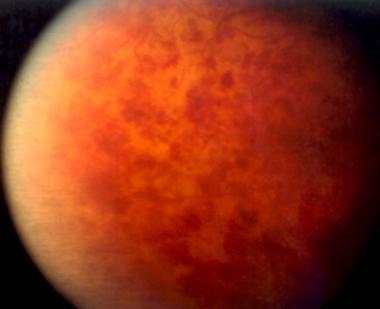
Recent onset central retinal vein occlusion, showing extensive hemorrhages in the posterior pole and giving the " blood and thunder appearance."
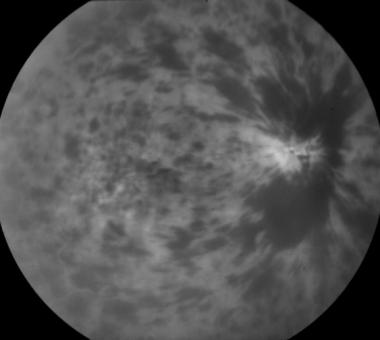
Peripheral fundus view of the same patient with central retinal vein occlusion as in the previous image, showing hemorrhages extending all over the fundus.
Fluorescein angiograph of same patient with central retinal vein occlusion as in previous images, showing hypofluorescence due to blockage from hemorrhages in the retina. It is not useful to perform a fluorescein angiogram in acute stages of the disease.
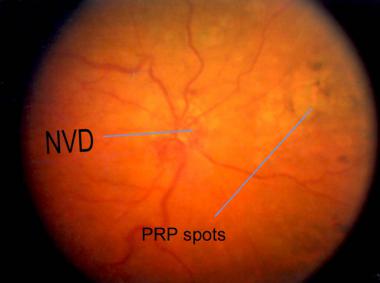
Fundus picture of the same patient with central retinal vein occlusion as in previous images, showing resolving neovascularization of the disc and panretinal photocoagulation scars.
Fluorescein angiogram of the same patient with central retinal vein occlusion as in the previous images, taken more than 1 year later, showing persistent cystoid macular edema with good laser spots. In view of the devastating complications associated with the severe form of CRVO, a number of classifications were described in the literature. All of these classifications take into account the area of retinal capillary nonperfusion and the development of neovascular complications. [1, 2, 3, 4, 5]
Broadly, CRVO can be divided into 2 clinical types, ischemic and nonischemic. In addition, a number of patients may have an intermediate presentation with variable clinical course. On initial presentation, it may be difficult to classify a given patient into either category, since CRVO may change with time.
A number of clinical and ancillary investigative factors are taken into account for classifying CRVO, including vision at presentation, presence or absence of relative afferent pupillary defect, extent of retinal hemorrhages, cotton-wool spots, extent of retinal perfusion by fluorescein angiography, and electroretinographic changes.
Nonischemic CRVO is the milder form of the disease. It may present with good vision, few retinal hemorrhages and cotton-wool spots, no relative afferent pupillary defect, and good perfusion to the retina. Nonischemic CRVO may resolve fully with good visual outcome or may progress to the ischemic type. Note the images below.
Patient with nonischemic central retinal vein occlusion presented with dilated, tortuous veins and superficial hemorrhages.
Fundus picture of the same patient with central retinal vein occlusion as in previous image, showing resolved hemorrhages and pigmentary changes in the macula several months later. Ischemic CRVO is the severe form of the disease. CRVO may present initially as the ischemic type, or it may progress from nonischemic. Usually, ischemic CRVO presents with severe visual loss, extensive retinal hemorrhages and cotton-wool spots, presence of relative afferent pupillary defect, poor perfusion to retina, and presence of severe electroretinographic changes. In addition, patients may end up with neovascular glaucoma and a painful blind eye. Pathophysiology
The exact pathogenesis of the thrombotic occlusion of the central retinal vein is not known. Various local and systemic factors play a role in the pathological closure of the central retinal vein. [3, 6, 7]
The central retinal artery and vein share a common adventitial sheath as they exit the optic nerve head and pass through a narrow opening in the lamina cribrosa. Because of this narrow entry in the lamina cribrosa, the vessels are in a tight compartment with limited space for displacement. This anatomical position predisposes to thrombus formation in the central retinal vein by various factors, including slowing of the blood stream, changes in the vessel wall, and changes in the blood.
Arteriosclerotic changes in the central retinal artery transform the artery into a rigid structure and impinge upon the pliable central retinal vein, causing hemodynamic disturbances, endothelial damage, and thrombus formation. This mechanism explains the fact that there may be an associated arterial disease with central retinal vein occlusion (CRVO). However, this association has not been proven consistently, and various authors disagree on this fact.
Thrombotic occlusion of the central retinal vein can occur as a result of various pathologic insults, including compression of the vein (mechanical pressure due to structural changes in lamina cribrosa, eg, glaucomatous cupping, inflammatory swelling in optic nerve, orbital disorders); hemodynamic disturbances (associated with hyperdynamic or sluggish circulation); vessel wall changes (eg, vasculitis); and changes in the blood (eg, deficiency of thrombolytic factors, increase in clotting factors).
Occlusion of the central retinal vein leads to the backup of the blood in the retinal venous system and increased resistance to venous blood flow. This increased resistance causes stagnation of the blood and ischemic damage to the retina. It has been postulated that ischemic damage to the retina stimulates increased production of vascular endothelial growth factor (VEGF) in the vitreous cavity. Increased levels of VEGF stimulate neovascularization of the posterior and anterior segment (responsible for secondary complications due to CRVO). Also, it has been shown that VEGF causes capillary leakage leading to macular edema (which is the leading cause of visual loss in both ischemic CRVO and nonischemic CRVO).
The prognosis of CRVO depends upon the reestablishment of patency of the venous system by recanalization, dissolution of clot, or formation of optociliary shunt vessels. Epidemiology Frequency United States Central retinal vein occlusion (CRVO) and branch retinal vein occlusion constitute the second most common retinal vascular disorder. The nonischemic type is more common than the ischemic type.
In a recent publication, the Beaver Dam Eye Study Group reported the 15-year cumulative incidence of CRVO to be 0.5%. [8] International A large population-based study in Israel reported a 4-year incidence of retinal vein occlusion of 2.14 cases per 1000 of general population older than 40 years and 5.36 cases per 1000 of general population older than 64 years.
In Australia, the prevalence of vein occlusion ranges from 0.7% in patients aged 49-60 years to 4.6% in patients older than 80 years. [9] Mortality/Morbidity CRVO is not associated directly with increased mortality. Nonischemic CRVO may resolve completely without any complications in about 10% of cases. In about 50% of patients, vision may be 20/200 or worse. One third of patients may progress to the ischemic type, commonly in the first 6-12 months after presentation.
In more than 90% of patients with ischemic CRVO, final visual acuity may be 20/200 or worse. Anterior segment neovascularization with associated neovascular glaucoma develops in more than 60% of cases. This can happen within a few weeks and up to 1-2 years afterward.
It has been reported that the fellow eye may develop retinal vein occlusion in about 7% of cases within 2 years. In another report, the 4-year risk of developing second venous occlusion is 2.5% in the same eye and 11.9% in the fellow eye. Neovascular glaucoma may result in a painful blind eye. Race CRVO does not have any particular racial preference. Sex CRVO occurs slightly more frequently in males than in females. Age More than 90% of CRVO occurs in patients older than 50 years, but it has been reported in all age groups.
History A direct review of systems toward the various systemic and local factors predisposing the central retinal vein occlusion (CRVO) is indicated.
Significant history includes the following: · Hypertension · Diabetes mellitus · Cardiovascular disorders · Bleeding or clotting disorders · Vasculitis · Autoimmune disorders · Use of oral contraceptives · Closed-head trauma · Alcohol consumption · Amount of physical activity · Primary open-angle glaucoma or angle-closure glaucoma
Ocular symptoms at initial presentation are as follows: · Asymptomatic · Decreased vision · Visual loss can be sudden or gradual, over a period of days to weeks. Visual loss ranges from mild to severe. Patients can present with transient obscurations of vision initially, later progressing to constant visual loss. · Photophobia · Painful blind eye · Redness of eyes
Ocular symptoms in later stages are as follows: · Decrease of vision · Pain in the eyes · Discomfort · Redness · Watering
Physical Patients with central retinal vein occlusion (CRVO) should undergo a complete eye examination, including visual acuity, pupillary reactions, slit lamp examination of the anterior and posterior segments, undilated examination of the iris, gonioscopy, fundus examination with indirect ophthalmoscope, and fundus contact lens. [10] Note the following: · Visual acuity: Best-corrected vision always should be obtained. It is one of the important indicators of the final visual prognosis. · Pupillary reactions may be normal and may present with relative afferent pupillary reflex. If the iris has abnormal blood vessels, the pupil may not react. · Conjunctiva: Advanced stages may show congestion on conjunctival and ciliary vessels. · Cornea: Advanced stages may show diffuse corneal edema obscuring the visibility of internal structures. · The iris may be normal. Advanced stages may show neovascularization. These vessels are detected best on an undilated iris. Initially, the vessels may be seen around pupillary margins and peripheral iridectomy openings if present. · The anterior chamber angle is examined by gonioscopy. This is examined best in an undilated iris. Initially, it may show neovascularization with open angles and later show total peripheral anterior synechia and closed angles. · Fundus examination: Retinal hemorrhages may present in all 4 quadrants. Hemorrhages can be superficial, dot and blot, and/or deep. In some patients, hemorrhages may be seen in the peripheral fundus only. Hemorrhages can be mild to severe, covering the whole fundus and giving a " blood and thunder appearance." Note the images below.
Scattered retinal hemorrhages in a patient with central retinal vein occlusion.
Fundus of a patient with nonischemic central retinal vein occlusion, showing few scattered peripheral fundus hemorrhages.
Recent onset central retinal vein occlusion, showing extensive hemorrhages in the posterior pole and giving the " blood and thunder appearance." · Dilated tortuous veins: Veins may be dilated and tortuous, as shown in the image below.
Patient with nonischemic central retinal vein occlusion presented with dilated, tortuous veins and superficial hemorrhages. · Optic disc edema: The optic disc may be swollen during the early-stage disease. Note the images below.
Central retinal vein occlusion showing significant disc edema with dilated tortuous veins and scattered retinal hemorrhages.
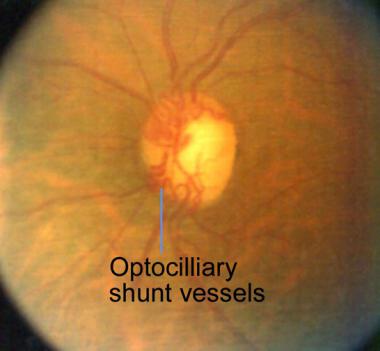
Fluorescein angiogram of the same patient with central retinal vein occlusion in as in previous image, showing leakage from disc, staining of retinal veins. · Cotton-wool spots are more common with ischemic CRVO. Usually, they are concentrated around the posterior pole. Cotton-wool spots may resolve in 2-4 months. · Neovascularization of the disc: Fine abnormal neovascularization of the disc (NVD) or within 1 disc diameter from the disc may be present. NVD indicates severe ischemia of the retina. NVD is sometimes difficult to differentiate from optociliary shunt vessels. NVD can lead to preretinal or vitreous hemorrhage. · Neovascularization elsewhere: Neovascularization elsewhere (NVE) is not as common as NVD. NVE indicates severe ischemia of the retina. NVE can lead to preretinal or vitreous hemorrhage. · Optociliary shunt vessels (depicted in the images below) are abnormal blood vessels on the disc, directing blood from retinal circulation to choroidal circulation, which indicate good compensatory circulation.
Fundus picture of a well-compensated, old central retinal vein occlusion showing optociliary shunt vessels.
Red-free photo of the same patient with central retinal vein occlusion as in the previous image, showing prominent optociliary shunt vessels. · Preretinal or vitreous hemorrhage · Macular edema with or without exudates · Cystoid macular edema · Lamellar or full-thickness macular hole · Optic atrophy · Pigmentary changes in the macula Causes Central retinal vein obstruction has been associated with various systemic pathological conditions, although the exact cause and effect relationship has not been proven.
Some of the conditions in which CRVO has been associated include the following: · Systemic vascular disease - Hypertension, diabetes mellitus, cardiovascular disease · Blood dyscrasias - Polycythemia vera, lymphoma, leukemia · Clotting disorders - Activated protein C resistance, lupus anticoagulant, anticardiolipin antibodies, protein C, protein S, antithrombin III · Paraproteinemia and dysproteinemias - Multiple myeloma, cryoglobulinemia · Vasculitis - Syphilis, sarcoidosis · Autoimmune disease - Systemic lupus erythematosus · Oral contraceptive use in women · Obstructive sleep apnea - This affects more patients with retinal vein obstruction than other disorders; treatment of the sleep apnea may help prevent central vein obstruction. [11] · Other rare associations - Closed-head trauma, optic disc drusen, arteriovenous malformations of retina
The Eye Disease Case-Control Study Group reported that the risk of CRVO is decreased in men with increasing levels of physical activity and increasing levels of alcohol consumption. The same study group reported a decreased risk of CRVO with the use of postmenopausal estrogens and an increased risk with higher erythrocyte sedimentation rates in women.
Differential Diagnoses · Branch Retinal Vein Occlusion · Ocular Ischemic Syndrome
Workup
Laboratory Studies No laboratory studies are routinely indicated in the diagnosis of central retinal vein occlusion (CRVO). In older patients, laboratory testing should be directed toward identifying systemic vascular problems. In young patients, laboratory testing may be tailored depending upon individual findings, to include the following: · Complete blood cell (CBC) count · Glucose tolerance test · Lipid profile · Serum protein electrophoresis · Chemistry profile · Hematologic tests · Syphilis serology · In addition, thrombophilic screening, activated protein C resistance, lupus anticoagulant, anticardiolipin antibodies, protein C, protein S, and antithrombin III may be completed. Imaging Studies Color Doppler imaging is a noninvasive quantitative method of assessing the retrobulbar circulation. Detection of low venous velocities has been used to predict the onset of iris neovascularization. At present, this is performed as an investigational procedure in large facilities. [12] Optical coherence tomography (OCT) [13] scanning is a noninvasive, noncontact, transpupillary imaging technology that can image retinal structures in vivo with an axial resolution of 1-15 µm. OCT quantitatively measures the retinal thickness in micrometers in situ and in real time. OCT can detect even subtle macular edema in the presence of significant hemorrhages, which may not be evident on fluorescein angiography because of blockage from hemorrhage. OCT is used exclusively to monitor macular edema over time and the response with various treatment modalities. [13, 14] Other Tests Fluorescein angiography Fluorescein angiography is the most useful test for the evaluation of retinal capillary nonperfusion, posterior segment neovascularization, and macular edema. [2] Note the images below.
Fluorescein angiogram of a patient with nonischemic central retinal vein occlusion, showing staining of dilated tortuous veins with leakage into macula in a cystoid pattern.
Fluorescein angiogram of the same patient as in previous image, showing perifoveal capillary leakage in a cystoid pattern in late phases of angiogram.
Late phase of fluorescein angiograph of the same patient as in previous image, showing cystoid pattern of leakage from perifoveal dilated leaking capillary network. Fluorescein angiography is one of the tests used in the classification of CRVO. Areas of capillary nonperfusion are visualized as hypofluorescence, but hemorrhages can block fluorescence and give a similar picture. Therefore, in the early stages of the disease process, due to extensive hemorrhages, fluorescein angiography gives little information regarding the perfusion status of the retina. Once the hemorrhages clear, areas of capillary nonperfusion can be detected as hypofluorescence in the fluorescein angiography.
Various studies have reported different criteria for defining ischemic CRVO versus nonischemic CRVO based on the extent of capillary nonperfusion of the retina. The amount of retinal nonperfusion ranges from 10-30 disc areas. In addition, fluorescein angiography may show delayed arteriovenous transit, staining along the retinal veins, microaneurysms, arteriovenous collaterals, NVD, NVE, and dilated optic nerve head capillaries.
In a nonischemic central retinal vein obstruction, angiography may show minimal or absent retinal capillary nonperfusion, staining along the retinal veins, microaneurysms, and dilated optic nerve head capillaries. Resolved CRVO may be completely normal.
Macular edema may be detected as leakage from perifoveal capillaries (depicted in the image below), leakage from microaneurysms, or diffuse leakage on fluorescein angiography. If extensive edema is present, fluorescein angiography may show pooling of dye in large cystoid spaces. In addition, capillary nonperfusion around the fovea may indicate macular ischemia. If macular edema persists, pigmentary changes become evident.
Arteriovenous phase of fluorescein angiograph showing perifoveal capillary leakage in a patient with nonischemic central retinal vein occlusion. Electroretinography Electroretinography (ERG) is another useful test to evaluate the functional status of the retina and to classify CRVO. [13, 16, 17] In ERG waveform, b-wave and a-wave are produced by the inner retina and the outer retina, respectively. In central retinal vein obstruction, perfusion of the inner retina is affected, so that the amplitude of the b-wave is decreased relative to the a-wave; the b-to-a ratio has been shown to be reduced. Some studies indicate that a b-to-a ratio of less than 1 suggests an ischemic central retinal vein obstruction. Histologic Findings
Not many histopathologic reports exist in the literature. A report of histologic sections of 29 eyes with central retinal vein obstruction showed a fresh or recanalized thrombus at or just posterior to the lamina cribrosa. Within the thrombi, a mild lymphocytic infiltration with prominent endothelial cells was seen. Loss of the inner retinal layers consistent with inner retinal ischemia also was seen. [18]
Treatment & Management Approach Considerations No known effective medical treatment is available for either the prevention of or the treatment of central retinal vein occlusion (CRVO). Identifying and treating any systemic medical problems to reduce further complications is important. Because the exact pathogenesis of the CRVO is not known, various medical modalities of treatment have been advocated by multiple authors with varying success in preventing complications and in preserving vision.
Macular edema is one of the prominent treatable causes of decreased visual acuity in patients with CRVO. The exact mechanism of macular edema is unclear, but multiple factors involved include increased venous pressure, elevated levels of VEGF, and deregulation of multiple inflammatory mediators leading to increased capillary permeability and leakage. Various treatment modalities have been used to counter different components of macular edema pathogenesis, with significant progress in stabilizing or improving visual acuity.
Advocated treatments are as follows: · Aspirin · Anti-inflammatory agents · Isovolemic hemodilution · Plasmapheresis · Systemic anticoagulation with warfarin, heparin, and alteplase · Fibrinolytic agents · Systemic corticosteroids · Local anticoagulation with intravitreal injection of alteplase · Intravitreal injection of ranibizumab · Intravitreal injection of aflibercept · Intravitreal injection of triamcinolone · Intravitreal injection of bevacizumab · Dexamethasone intravitreal implant
The Ophthalmic Technology Assessment Committee Retina/Vitreous panel of the American Academy of Ophthalmology evaluated available literature regarding efficacy of available pharmacotherapies in the treatment of macular edema due to CRVO. The panel reported that intravitreal anti-VEGF therapy is safe and effective over 2 years for macular edema and that delayed treatment is associated with worse visual outcomes. Intravitreal corticosteroid therapy yielded short-term efficacy but was associated with a higher frequency of adverse events. [19]
Medical Care Corticosteroid therapy Intraocular steroid injection has been shown to be effective in decreasing macular edema. Although the exact mechanism of action is unknown, steroids work by targeting various inflammatory pathways and decreasing expression of VEGF, reducing vascular permeability, stabilizing endothelial tight junctions, and decreasing macular edema.
Currently, triamcinolone acetonide and dexamethasone are the two steroid preparations used to treat macular edema associated with central retinal vein occlusion (CRVO).
Surgical Care Laser photocoagulation Laser photocoagulation is the known treatment of choice in the treatment of various complications associated with retinal vascular diseases (eg, diabetic retinopathy, branch retinal vein occlusion). Panretinal photocoagulation (PRP) has been used in the treatment of neovascular complications of central retinal vein occlusion (CRVO) for a long time. However, no definite guidelines exist regarding exact indication and timing of PRP. A National Eye Institute (NEI) sponsored multicenter prospective study, the Central Vein Occlusion Study (CVOS), provided guidelines for the treatment and follow-up care of patients with CRVO. [1, 10, 36, 37, 38]
CVOS evaluated the efficacy of prophylactic PRP in eyes with 10 or more disc areas of retinal capillary nonperfusion, confirmed by fluorescein angiography, in preventing development of 2 clock hours of iris neovascularization or any angle neovascularization or whether it is more appropriate to apply PRP only when iris neovascularization or any angle neovascularization occurs. CVOS concluded that prophylactic PRP did not prevent the development of iris neovascularization and recommended to wait for the development of early iris neovascularization and then apply PRP.
Argon green laser usually is used. Laser parameters should be about 500-µm size, 0.1-0.2 second duration, and power should be sufficient to give medium white burns. Laser spots are applied around the posterior pole, extending anterior to equator. They should be about 1 burn apart and total 1200-2500 spots.
If ocular media is hazy for laser to be applied, cryoablation of the peripheral fundus is performed. About 16-32 transscleral cryo spots are applied from ora serrata posteriorly.
CVOS evaluated the efficacy of macular grid photocoagulation in preserving or improving central visual acuity in eyes with macular edema due to central vein occlusion (CVO) and best-corrected visual acuity of 20/50 or poorer. Macular grid photocoagulation was effective in reducing angiographic evidence of macular edema, but it did not improve visual acuity in eyes with reduced vision due to macular edema from CVO. At present, the results of this study do not support a recommendation for macular grid photocoagulation for macular edema. Radial optic neurotomy Radial optic neurotomy (RON) [44, 45, 46, 47, 48, 49] is a new surgical technique in which a microvitreoretinal blade is used during pars plana vitrectomy to relax the scleral ring around the optic nerve. The central retinal artery and vein passes through the narrow openings of the cribriform plate in the optic disc.
Promoters of this technique suggest that CRVO may be due to the compression of the central retinal vein at this location creating a compartment syndrome. If this procedure is successful, it decompresses the closed compartment and leads to an improvement in venous outflow and a reduction of macular edema.
In one recent study, RON resulted in clinically relevant improvements on a long-term basis. Patients with nonischemic CRVO may respond more favorably than patients with ischemic CRVO.
In another study, significant improvements were observed in the b-to-a ratio of the standard combined ERG after surgery in eyes with CRVO.
The benefits from surgery have not been clearly documented. One study, looking into the biomechanical effect of RON, found negligible change in the space around the central retinal vein; RON is unlikely to be a procedure that could mechanically ameliorate the clinical sequelae of a central vein occlusion. The improvement of retinal function is most likely due to improved oxygenation of the retina caused by vitrectomy and not by RON.
In addition to the regular complications of vitrectomy, RON can result in significant hemorrhage and neovascularization at the incision site.
No consensus currently exists among various researchers regarding the exact criteria for the use of RON. Vitrectomy A vitrectomy [50] is a technique in which the vitreous is surgically removed along with removal of the posterior hyaloid.
Some studies have shown that a vitrectomy may be beneficial for macular edema due to CRVO. One theory is that a vitrectomy may relieve traction on the macula and, thus, reduce macular edema. According to another hypothesis, removing the vitreous will also remove cytokines and VEGF associated with a venous occlusive event; thus, the stimulus for macular edema will be reduced.
At the present time, no convincing evidence indicates that a vitrectomy is the best approach.
Consultations A general ophthalmologist should consult a retinal specialist for management of CRVO complications. Other consults include an internist for proper evaluation and management of any systemic medical problems. If patients develop neovascular glaucoma, a glaucoma specialist should be consulted. Diet Diet should be tailored to systemic medical problems.
Activity No restrictions usually exist. If patients develop vitreous hemorrhage, they are advised to avoid strenuous activities, sleep with few pillows, and avoid bending and lifting heavy weights.
Medication Medication Summary
The goals of pharmacotherapy are to reduce morbidity and to prevent complications.
Class Summary These agents bind to VEGF-A receptors to arrest macular edema and improve visual acuity associated with CVRO. Ranibizumab (Lucentis) VEGF antibody. Indicated for macular edema following retinal vein occlusion. Aflibercept intravitreal (Eylea) Binds and prevents activation of vascular endothelial growth factors (VEGF-A) and placental growth factor (PIGF). Activation of VEGF-A and PIGF can result in neovascularization and vascular permeability. It is indicated for treatment of macular edema following retinal vein occlusion (branched or central retinal vein occlusion). Bevacizumab (Avastin) Bevacizumab (Avastin, Genentech, Inc.) is a recombinant, humanized monoclonal antibody that binds all isoforms of VEGF-A. It is used as an off-label medication in various ocular conditions associated with up-regulation of VEGF and increased vascular permeability and neovascularization. Corticosteroids Class Summary These agents have anti-inflammatory properties and cause profound and varied metabolic effects. Corticosteroids modify the body's immune response to diverse stimuli. Follow-up Further Outpatient Care
Since neovascular complications and development of second venous occlusions can develop after central retinal vein occlusion (CRVO), all of these patients need follow-up care for long periods of time.
CVOS recommended careful observation with frequent follow-up examinations in the early months for detection of iris neovascularization and prompt treatment.
Patients with poor initial visual acuity should be monitored every month during the first few months and spaced thereafter, depending on the course of the disease. These criteria apply more for patients with ischemic CRVO than with patients with nonischemic CRVO.
With any associated complications, follow-up care should be individualized. Deterrence/Prevention
Optimal control of associated systemic diseases may reduce the incidence of similar occlusions in the fellow eye.
Even though controversial, good control of intraocular pressure in patients known to have glaucoma may prevent CRVO. Complications Ocular neovascularization is a potential complication. [33] Anterior segment neovascularization can lead to neovascular glaucoma. Posterior segment neovascularization can lead to vitreous hemorrhage.
Macular edema is another potential complication. [51, 38, 52] Macular edema is the common cause of decreased vision in CRVO, more so in the nonischemic type. It may resolve with good visual return. The patient may develop permanent degenerative changes with poor visual prognosis and may develop cystoid macular edema leading to lamellar or full-thickness macular hole.
Other potential complications include cellophane maculopathy and macular pucker, as well as optic atrophy.
Reported complications due to treatment with intravitreal injections include endophthalmitis, vitreous hemorrhage, and retinal detachment.
Prognosis For nonischemic CRVO, complete recovery with good visual recovery occurs only in about 10% of cases. Fifty percent of patients will have 20/200 or worse vision. About one third of patients convert to ischemic CRVO. CVOS noted that, of 547 eyes initially diagnosed to have nonischemic central retinal vein obstructions, 185 (34%) progressed to become ischemic central retinal vein obstructions within 3 years; 15% converted within the first 4 months.
For ischemic CRVO, more than 90% of patients will have 20/200 or worse vision. About 60% of patients develop ocular neovascularization with associated complications. About 10% of patients can develop CRVO or other type of vein occlusions within either the same eye or the contralateral eye within 2 years.
The long-term prognosis of CRVO has significantly improved with new anti-VEGF agents and steroids, maintaining good visual acuity for a long duration in most patients, except those with severe ischemic maculopathy. Development of neovascular complications has also decreased with continued monitoring and anti–VEGF treatment.
Patient Education Good control of systemic medical problems is important, as are regular medical and ophthalmologic checkups.
References 1. Central Vein Occlusion Study Group. Natural history and clinical management of central retinal vein occlusion. [published erratum appears in Arch Ophthalmol 1997 Oct; 115(10): 1275]. Arch Ophthalmol. 1997 Apr. 115(4): 486-91. [Medline]. 2. Hayreh SS. Classification of central retinal vein occlusion. Ophthalmology. 1983 May. 90(5): 458-74. [Medline]. 3. Hayreh SS. Retinal vein occlusion. Indian J Ophthalmol. 1994 Sep. 42(3): 109-32. [Medline]. 4. Hayreh SS, Zimmerman MB, Podhajsky P. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. Am J Ophthalmol. 1994 Apr 15. 117(4): 429-41. [Medline]. 5. Williamson TH. Central retinal vein occlusion: what's the story?. Br J Ophthalmol. 1997 Aug. 81(8): 698-704. [Medline]. 6. David R, Zangwill L, Badarna M, et al. Epidemiology of retinal vein occlusion and its association with glaucoma and increased intraocular pressure. Ophthalmologica. 1988. 197(2): 69-74. [Medline]. 7. Ota M, Tsujikawa A, Kita M, et al. Integrity of foveal photoreceptor layer in central retinal vein occlusion. Retina. 2008 Nov-Dec. 28(10): 1502-8. [Medline]. 8. Klein R, Moss SE, Meuer SM, et al. The 15-year cumulative incidence of retinal vein occlusion: the Beaver Dam Eye Study. Arch Ophthalmol. 2008 Apr. 126(4): 513-8. [Medline]. 9. Mitchell P, Smith W, Chang A. Prevalence and associations of retinal vein occlusion in Australia. The Blue Mountains Eye Study. Arch Ophthalmol. 1996 Oct. 114(10): 1243-7. [Medline]. 10. Central Vein Occlusion Study Group. Baseline and early natural history report. Arch Ophthalmol. 1993 Aug. 111(8): 1087-95. [Medline]. 11. Glacet-Bernard A, les Jardins GL, Lasry S, Coscas G, Soubrane G, Souied E, et al. Obstructive sleep apnea among patients with retinal vein occlusion. Arch Ophthalmol. 2010 Dec. 128(12): 1533-8. [Medline]. 12. Baxter GM, Williamson TH. Color Doppler flow imaging in central retinal vein occlusion: a new diagnostic technique?. Radiology. 1993 Jun. 187(3): 847-50. [Medline]. 13. Moschos MM, Moschos M. Intraocular bevacizumab for macular edema due to CRVO. A multifocal-ERG and OCT study. Doc Ophthalmol. 2008 Mar. 116(2): 147-52. [Medline]. 14. Gupta B, Grewal J, Adewoyin T, et al. Diurnal variation of macular oedema in CRVO: prospective study. Graefes Arch Clin Exp Ophthalmol. 2008 Dec 4. [Medline]. 15. Kashani AH, Lee SY, Moshfeghi A, Durbin MK, Puliafito CA. OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY OF RETINAL VENOUS OCCLUSION. Retina. 2015 Nov. 35 (11): 2323-31. [Medline]. [Full Text]. 16. Breton ME, Quinn GE, Keene SS, et al. Electroretinogram parameters at presentation as predictors of rubeosis in central retinal vein occlusion patients. Ophthalmology. 1989 Sep. 96(9): 1343-52. [Medline]. 17. Sato E, Yamamoto S, Ogata K, et al. Changes of electroretinogram without improvement of retinal circulation after radial optic neurotomy for central retinal vein occlusion. ERG changes after RON for CRVO. Doc Ophthalmol. 2008 Mar. 116(2): 153-8. [Medline]. 18. Green WR, Chan CC, Hutchins GM. Central retinal vein occlusion: a prospective histopathologic study of 29 eyes in 28 cases. Retina. 1981. 1: 27-55. 19. Yeh S, Kim SJ, Ho AC, Schoenberger SD, Bakri SJ, Ehlers JP, et al. Therapies for macular edema associated with central retinal vein occlusion: a report by the American Academy of Ophthalmology. Ophthalmology. 2015 Apr. 122 (4): 769-78. [Medline]. [Full Text]. 20. Ip MS, Scott IU, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 5. Arch Ophthalmol. 2009 Sep. 127(9): 1101-14. [Medline]. [Full Text]. 21. Aref AA, Scott IU, Oden NL, Ip MS, Blodi BA, VanVeldhuisen PC, et al. Incidence, Risk Factors, and Timing of Elevated Intraocular Pressure After Intravitreal Triamcinolone Acetonide Injection for Macular Edema Secondary to Retinal Vein Occlusion: SCORE Study Report 15. JAMA Ophthalmol. 2015 Sep. 133 (9): 1022-9. [Medline]. [Full Text]. 22. Haller JA, Bandello F, Belfort R Jr, et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010 Jun. 117(6): 1134-1146.e3. [Medline]. 23. Brown DM, Campochiaro PA, Singh RP, Li Z, Gray S, Saroj N, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010 Jun. 117(6): 1124-1133.e1. [Medline]. 24. Kinge B, Stordahl PB, Forsaa V, Fossen K, Haugstad M, Helgesen OH, et al. Efficacy of ranibizumab in patients with macular edema secondary to central retinal vein occlusion: results from the sham-controlled ROCC study. Am J Ophthalmol. 2010 Sep. 150(3): 310-4. [Medline]. 25. Varma R, Bressler NM, Suñ er I, Lee P, Dolan CM, Ward J, et al. Improved Vision-Related Function after Ranibizumab for Macular Edema after Retinal Vein Occlusion: Results from the BRAVO and CRUISE Trials. Ophthalmology. 2012 Jul 17. [Medline]. 26. Spaide RF, Chang LK, Klancnik JM, et al. Prospective Study of Intravitreal Ranibizumab as a Treatment for Decreased Visual Acuity Secondary to Central Retinal Vein Occlusion. Am J Ophthalmol. 2008 Oct 17. [Medline]. 27. Heier JS, Campochiaro PA, Yau L, Li Z, Saroj N, Rubio RG, et al. Ranibizumab for macular edema due to retinal vein occlusions: long-term follow-up in the HORIZON trial. Ophthalmology. 2012 Apr. 119 (4): 802-9. [Medline]. [Full Text]. 28. Larsen M, Waldstein SM, Boscia F, Gerding H, Moné s J, Tadayoni R, et al. Individualized Ranibizumab Regimen Driven by Stabilization Criteria for Central Retinal Vein Occlusion: Twelve-Month Results of the CRYSTAL Study. Ophthalmology. 2016 May. 123 (5): 1101-11. [Medline]. [Full Text]. 29. Boyer D, Heier J, Brown DM, Clark WL, Vitti R, Berliner AJ, et al. Vascular endothelial growth factor Trap-Eye for macular edema secondary to central retinal vein occlusion: six-month results of the phase 3 COPERNICUS study. Ophthalmology. 2012 May. 119(5): 1024-32. [Medline]. 30. Ogura Y, Roider J, Korobelnik JF, Holz FG, Simader C, Schmidt-Erfurth U, et al. Intravitreal aflibercept for macular edema secondary to central retinal vein occlusion: 18-month results of the phase 3 GALILEO study. Am J Ophthalmol. 2014 Nov. 158 (5): 1032-8. [Medline]. [Full Text]. 31. Korobelnik JF, Holz FG, Roider J, Ogura Y, Simader C, Schmidt-Erfurth U, et al. Intravitreal Aflibercept Injection for Macular Edema Resulting from Central Retinal Vein Occlusion: One-Year Results of the Phase 3 GALILEO Study. Ophthalmology. 2014 Jan. 121 (1): 202-8. [Medline]. [Full Text]. 32. Heier JS, Clark WL, Boyer DS, Brown DM, Vitti R, Berliner AJ, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: two-year results from the COPERNICUS study. Ophthalmology. 2014 Jul. 121 (7): 1414-1420.e1. [Medline]. [Full Text]. 33. Batioglu F, Astam N, Ozmert E. Rapid improvement of retinal and iris neovascularization after a single intravitreal bevacizumab injection in a patient with central retinal vein occlusion and neovascular glaucoma. Int Ophthalmol. 2008 Feb. 28(1): 59-61. [Medline]. 34. Kriechbaum K, Michels S, Prager F, et al. Intravitreal Avastin for macular oedema secondary to retinal vein occlusion: a prospective study. Br J Ophthalmol. 2008 Apr. 92(4): 518-22. [Medline]. 35. Epstein DL, Algvere PV, von Wendt G, Seregard S, Kvanta A. Benefit from bevacizumab for macular edema in central retinal vein occlusion: twelve-month results of a prospective, randomized study. Ophthalmology. 2012 Dec. 119 (12): 2587-91. [Medline]. 36. Central Vein Occlusion Study Group. A randomized clinical trial of early panretinal photocoagulation for ischemic central vein occlusion. The Central Vein Occlusion Study Group N report. Ophthalmology. 1995 Oct. 102(10): 1434-44. [Medline]. 37. Central Vein Occlusion Study Group. Central vein occlusion study of photocoagulation therapy. Baseline findings. Online J Curr Clin Trials. 1993 Oct 14. Doc No 95: [Medline]. 38. Central Vein Occlusion Study Group. Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. The Central Vein Occlusion Study Group M report. Ophthalmology. 1995 Oct. 102(10): 1425-33. [Medline]. 39. Browning DJ, Rotberg MH. Vitreous Hemorrhage complicating laser-induced chorioretinal anastomosis for central retinal vein occlusion. Am J Ophthalmol. 1996 Oct. 122(4): 588-9. [Medline]. 40. Eccarius SG, Moran MJ, Slingsby JG. Choroidal neovascular membrane after laser-induced chorioretinal anastomosis. Am J Ophthalmol. 1996 Oct. 122(4): 590-1. [Medline]. 41. Luttrull JK. Epiretinal membrane and traction retinal detachment complicating laser- induced chorioretinal venous anastomosis. Am J Ophthalmol. 1997 May. 123(5): 698-9. [Medline]. 42. McAllister IL, Constable IJ. Laser-induced chorioretinal venous anastomosis for treatment of nonischemic central retinal vein occlusion. Arch Ophthalmol. 1995 Apr. 113(4): 456-62. [Medline]. 43. Mirshahi A, Roohipoor R, Lashay A, et al. Surgical induction of chorioretinal venous anastomosis in ischaemic central retinal vein occlusion: a non-randomised controlled clinical trial. Br J Ophthalmol. 2005 Jan. 89(1): 64-9. [Medline]. 44. Beck AP, Ryan EA, Lou PL, et al. Controversies regarding radial optic neurotomy for central retinal vein occlusion. Int Ophthalmol Clin. 2005 Fall. 45(4): 153-61. [Medline]. 45. Binder S, Aggermann T, Brunner S. Long-term effects of radial optic neurotomy for central retinal vein occlusion consecutive interventional case series. Graefes Arch Clin Exp Ophthalmol. 2007 Oct. 245(10): 1447-52. [Medline]. 46. Friberg TR, Smolinski P, Hill S, et al. Biomechanical assessment of radial optic neurotomy. Ophthalmology. 2008 Jan. 115(1): 174-80. [Medline]. 47. Opremcak EM, Bruce RA, Lomeo MD, et al. Radial optic neurotomy for central retinal vein occlusion: a retrospective pilot study of 11 consecutive cases. Retina. 2001. 21(5): 408-15. [Medline]. 48. Weizer JS, Stinnett SS, Fekrat S. Radial optic neurotomy as treatment for central retinal vein occlusion. Am J Ophthalmol. 2003 Nov. 136(5): 814-9. [Medline]. 49. Arevalo JF, Garcia RA, Wu L, et al. Radial optic neurotomy for central retinal vein occlusion: results of the Pan-American Collaborative Retina Study Group (PACORES). Retina. 2008 Oct. 28(8): 1044-52. [Medline]. 50. Leizaola-Fernandez C, Suarez-Tata L, Quiroz-Mercado H, et al. Vitrectomy with complete posterior hyaloid removal for ischemic central retinal vein occlusion: series of cases. BMC Ophthalmol. 2005 May 20. 5: 10. [Medline]. 51. Cekic O, Chang S, Tseng JJ, et al. Intravitreal triamcinolone treatment for macular edema associated with central retinal vein occlusion and hemiretinal vein occlusion. Retina. 2005 Oct-Nov. 25(7): 846-50. [Medline]. 52. Catier A, Tadayoni R, Paques M, et al. Characterization of macular edema from various etiologies by optical coherence tomography. Am J Ophthalmol. 2005 Aug. 140(2): 200-6. [Medline]. 53. (unpublished) A randomized, double-masked, sham-controlled phase 3 study of the efficacy, safety and tolerability of repeated intravitreal administration of VEGF trap-eye in subjects with macular edema secondary to central retinal vein occlusion (CRVO) (GALILEO). ClinicalTrials.gov Identifier: NCT01012973. 54. Bashshur ZF, Ma'luf RN, Allam S, et al. Intravitreal triamcinolone for the management of macular edema due to nonischemic central retinal vein occlusion. Arch Ophthalmol. 2004 Aug. 122(8): 1137-40. [Medline]. 55. Ip MS, Gottlieb JL, Kahana A, et al. Intravitreal triamcinolone for the treatment of macular edema associated with central retinal vein occlusion. Arch Ophthalmol. 2004 Aug. 122(8): 1131-6. [Medline]. 56. Patel PJ, Zaheer I, Karia N. Intravitreal triamcinolone acetonide for macular oedema owing to retinal vein occlusion. Eye. 2008 Jan. 22(1): 60-4. [Medline]. 57. Ramchandran RS, Fekrat S, Stinnett SS, et al. Fluocinolone acetonide sustained drug delivery device for chronic central retinal vein occlusion: 12-month results. Am J Ophthalmol. 2008 Aug. 146(2): 285-291. [Medline]. 58. Ferrara DC, Koizumi H, Spaide RF. Early bevacizumab treatment of central retinal vein occlusion. Am J Ophthalmol. 2007 Dec. 144(6): 864-71. [Medline]. 59. Epstein DL, Algvere PV, von Wendt G, Seregard S, Kvanta A. Bevacizumab for Macular Edema in Central Retinal Vein Occlusion: A Prospective, Randomized, Double-Masked Clinical Study. Ophthalmology. 2012 Mar 16. [Medline]. 60. Haller JA, et al. Intravitreal aflibercept injection (IAI) for macular edema secondary to branch retinal vein occlusion (BRVO): 24-week, results of the VIBRANT study. Presented at the 38th annual Macula Society meeting. Scottsdale, AZ. February 21, 2014.
Author Lakshmana M Kooragayala, MD
Specialty Editor Board Francisco Talavera, PharmD, PhD
Steve Charles, MD Chief Editor Douglas R Lazzaro, MD, FAAO, FACS Additional Contributors V Al Pakalnis, MD, PhD
https: //emedicine.medscape.com/article/1223746-overview#showall
Overview Background Central retinal vein occlusion (CRVO) is a common retinal vascular disorder. Clinically, CRVO presents with variable visual loss; the fundus may show retinal hemorrhages, dilated tortuous retinal veins, cotton-wool spots, macular edema, and optic disc edema. Note the images below.
Recent onset central retinal vein occlusion, showing extensive hemorrhages in the posterior pole and giving the " blood and thunder appearance."
Peripheral fundus view of the same patient with central retinal vein occlusion as in the previous image, showing hemorrhages extending all over the fundus.
Fluorescein angiograph of same patient with central retinal vein occlusion as in previous images, showing hypofluorescence due to blockage from hemorrhages in the retina. It is not useful to perform a fluorescein angiogram in acute stages of the disease.
Fundus picture of the same patient with central retinal vein occlusion as in previous images, showing resolving neovascularization of the disc and panretinal photocoagulation scars.
Fluorescein angiogram of the same patient with central retinal vein occlusion as in the previous images, taken more than 1 year later, showing persistent cystoid macular edema with good laser spots. In view of the devastating complications associated with the severe form of CRVO, a number of classifications were described in the literature. All of these classifications take into account the area of retinal capillary nonperfusion and the development of neovascular complications. [1, 2, 3, 4, 5]
Broadly, CRVO can be divided into 2 clinical types, ischemic and nonischemic. In addition, a number of patients may have an intermediate presentation with variable clinical course. On initial presentation, it may be difficult to classify a given patient into either category, since CRVO may change with time.
A number of clinical and ancillary investigative factors are taken into account for classifying CRVO, including vision at presentation, presence or absence of relative afferent pupillary defect, extent of retinal hemorrhages, cotton-wool spots, extent of retinal perfusion by fluorescein angiography, and electroretinographic changes.
Nonischemic CRVO is the milder form of the disease. It may present with good vision, few retinal hemorrhages and cotton-wool spots, no relative afferent pupillary defect, and good perfusion to the retina. Nonischemic CRVO may resolve fully with good visual outcome or may progress to the ischemic type. Note the images below.
Patient with nonischemic central retinal vein occlusion presented with dilated, tortuous veins and superficial hemorrhages.
Fundus picture of the same patient with central retinal vein occlusion as in previous image, showing resolved hemorrhages and pigmentary changes in the macula several months later. Ischemic CRVO is the severe form of the disease. CRVO may present initially as the ischemic type, or it may progress from nonischemic. Usually, ischemic CRVO presents with severe visual loss, extensive retinal hemorrhages and cotton-wool spots, presence of relative afferent pupillary defect, poor perfusion to retina, and presence of severe electroretinographic changes. In addition, patients may end up with neovascular glaucoma and a painful blind eye. Pathophysiology
The exact pathogenesis of the thrombotic occlusion of the central retinal vein is not known. Various local and systemic factors play a role in the pathological closure of the central retinal vein. [3, 6, 7]
The central retinal artery and vein share a common adventitial sheath as they exit the optic nerve head and pass through a narrow opening in the lamina cribrosa. Because of this narrow entry in the lamina cribrosa, the vessels are in a tight compartment with limited space for displacement. This anatomical position predisposes to thrombus formation in the central retinal vein by various factors, including slowing of the blood stream, changes in the vessel wall, and changes in the blood.
Arteriosclerotic changes in the central retinal artery transform the artery into a rigid structure and impinge upon the pliable central retinal vein, causing hemodynamic disturbances, endothelial damage, and thrombus formation. This mechanism explains the fact that there may be an associated arterial disease with central retinal vein occlusion (CRVO). However, this association has not been proven consistently, and various authors disagree on this fact.
Thrombotic occlusion of the central retinal vein can occur as a result of various pathologic insults, including compression of the vein (mechanical pressure due to structural changes in lamina cribrosa, eg, glaucomatous cupping, inflammatory swelling in optic nerve, orbital disorders); hemodynamic disturbances (associated with hyperdynamic or sluggish circulation); vessel wall changes (eg, vasculitis); and changes in the blood (eg, deficiency of thrombolytic factors, increase in clotting factors).
Occlusion of the central retinal vein leads to the backup of the blood in the retinal venous system and increased resistance to venous blood flow. This increased resistance causes stagnation of the blood and ischemic damage to the retina. It has been postulated that ischemic damage to the retina stimulates increased production of vascular endothelial growth factor (VEGF) in the vitreous cavity. Increased levels of VEGF stimulate neovascularization of the posterior and anterior segment (responsible for secondary complications due to CRVO). Also, it has been shown that VEGF causes capillary leakage leading to macular edema (which is the leading cause of visual loss in both ischemic CRVO and nonischemic CRVO).
The prognosis of CRVO depends upon the reestablishment of patency of the venous system by recanalization, dissolution of clot, or formation of optociliary shunt vessels. Epidemiology Frequency United States Central retinal vein occlusion (CRVO) and branch retinal vein occlusion constitute the second most common retinal vascular disorder. The nonischemic type is more common than the ischemic type.
In a recent publication, the Beaver Dam Eye Study Group reported the 15-year cumulative incidence of CRVO to be 0.5%. [8] International A large population-based study in Israel reported a 4-year incidence of retinal vein occlusion of 2.14 cases per 1000 of general population older than 40 years and 5.36 cases per 1000 of general population older than 64 years.
In Australia, the prevalence of vein occlusion ranges from 0.7% in patients aged 49-60 years to 4.6% in patients older than 80 years. [9] Mortality/Morbidity CRVO is not associated directly with increased mortality. Nonischemic CRVO may resolve completely without any complications in about 10% of cases. In about 50% of patients, vision may be 20/200 or worse. One third of patients may progress to the ischemic type, commonly in the first 6-12 months after presentation.
In more than 90% of patients with ischemic CRVO, final visual acuity may be 20/200 or worse. Anterior segment neovascularization with associated neovascular glaucoma develops in more than 60% of cases. This can happen within a few weeks and up to 1-2 years afterward.
It has been reported that the fellow eye may develop retinal vein occlusion in about 7% of cases within 2 years. In another report, the 4-year risk of developing second venous occlusion is 2.5% in the same eye and 11.9% in the fellow eye. Neovascular glaucoma may result in a painful blind eye. Race CRVO does not have any particular racial preference. Sex CRVO occurs slightly more frequently in males than in females. Age More than 90% of CRVO occurs in patients older than 50 years, but it has been reported in all age groups.
History A direct review of systems toward the various systemic and local factors predisposing the central retinal vein occlusion (CRVO) is indicated.
Significant history includes the following: · Hypertension · Diabetes mellitus · Cardiovascular disorders · Bleeding or clotting disorders · Vasculitis · Autoimmune disorders · Use of oral contraceptives · Closed-head trauma · Alcohol consumption · Amount of physical activity · Primary open-angle glaucoma or angle-closure glaucoma
Ocular symptoms at initial presentation are as follows: · Asymptomatic · Decreased vision · Visual loss can be sudden or gradual, over a period of days to weeks. Visual loss ranges from mild to severe. Patients can present with transient obscurations of vision initially, later progressing to constant visual loss. · Photophobia · Painful blind eye · Redness of eyes
Ocular symptoms in later stages are as follows: · Decrease of vision · Pain in the eyes · Discomfort · Redness · Watering
Physical Patients with central retinal vein occlusion (CRVO) should undergo a complete eye examination, including visual acuity, pupillary reactions, slit lamp examination of the anterior and posterior segments, undilated examination of the iris, gonioscopy, fundus examination with indirect ophthalmoscope, and fundus contact lens. [10] Note the following: · Visual acuity: Best-corrected vision always should be obtained. It is one of the important indicators of the final visual prognosis. · Pupillary reactions may be normal and may present with relative afferent pupillary reflex. If the iris has abnormal blood vessels, the pupil may not react. · Conjunctiva: Advanced stages may show congestion on conjunctival and ciliary vessels. · Cornea: Advanced stages may show diffuse corneal edema obscuring the visibility of internal structures. · The iris may be normal. Advanced stages may show neovascularization. These vessels are detected best on an undilated iris. Initially, the vessels may be seen around pupillary margins and peripheral iridectomy openings if present. · The anterior chamber angle is examined by gonioscopy. This is examined best in an undilated iris. Initially, it may show neovascularization with open angles and later show total peripheral anterior synechia and closed angles. · Fundus examination: Retinal hemorrhages may present in all 4 quadrants. Hemorrhages can be superficial, dot and blot, and/or deep. In some patients, hemorrhages may be seen in the peripheral fundus only. Hemorrhages can be mild to severe, covering the whole fundus and giving a " blood and thunder appearance." Note the images below.
Scattered retinal hemorrhages in a patient with central retinal vein occlusion.
Fundus of a patient with nonischemic central retinal vein occlusion, showing few scattered peripheral fundus hemorrhages.
Recent onset central retinal vein occlusion, showing extensive hemorrhages in the posterior pole and giving the " blood and thunder appearance." · Dilated tortuous veins: Veins may be dilated and tortuous, as shown in the image below.
Patient with nonischemic central retinal vein occlusion presented with dilated, tortuous veins and superficial hemorrhages. · Optic disc edema: The optic disc may be swollen during the early-stage disease. Note the images below.
Central retinal vein occlusion showing significant disc edema with dilated tortuous veins and scattered retinal hemorrhages.
Fluorescein angiogram of the same patient with central retinal vein occlusion in as in previous image, showing leakage from disc, staining of retinal veins. · Cotton-wool spots are more common with ischemic CRVO. Usually, they are concentrated around the posterior pole. Cotton-wool spots may resolve in 2-4 months. · Neovascularization of the disc: Fine abnormal neovascularization of the disc (NVD) or within 1 disc diameter from the disc may be present. NVD indicates severe ischemia of the retina. NVD is sometimes difficult to differentiate from optociliary shunt vessels. NVD can lead to preretinal or vitreous hemorrhage. · Neovascularization elsewhere: Neovascularization elsewhere (NVE) is not as common as NVD. NVE indicates severe ischemia of the retina. NVE can lead to preretinal or vitreous hemorrhage. · Optociliary shunt vessels (depicted in the images below) are abnormal blood vessels on the disc, directing blood from retinal circulation to choroidal circulation, which indicate good compensatory circulation.
Fundus picture of a well-compensated, old central retinal vein occlusion showing optociliary shunt vessels.
Red-free photo of the same patient with central retinal vein occlusion as in the previous image, showing prominent optociliary shunt vessels. · Preretinal or vitreous hemorrhage · Macular edema with or without exudates · Cystoid macular edema · Lamellar or full-thickness macular hole · Optic atrophy · Pigmentary changes in the macula Causes Central retinal vein obstruction has been associated with various systemic pathological conditions, although the exact cause and effect relationship has not been proven.
Some of the conditions in which CRVO has been associated include the following: · Systemic vascular disease - Hypertension, diabetes mellitus, cardiovascular disease · Blood dyscrasias - Polycythemia vera, lymphoma, leukemia · Clotting disorders - Activated protein C resistance, lupus anticoagulant, anticardiolipin antibodies, protein C, protein S, antithrombin III · Paraproteinemia and dysproteinemias - Multiple myeloma, cryoglobulinemia · Vasculitis - Syphilis, sarcoidosis · Autoimmune disease - Systemic lupus erythematosus · Oral contraceptive use in women · Obstructive sleep apnea - This affects more patients with retinal vein obstruction than other disorders; treatment of the sleep apnea may help prevent central vein obstruction. [11] · Other rare associations - Closed-head trauma, optic disc drusen, arteriovenous malformations of retina
The Eye Disease Case-Control Study Group reported that the risk of CRVO is decreased in men with increasing levels of physical activity and increasing levels of alcohol consumption. The same study group reported a decreased risk of CRVO with the use of postmenopausal estrogens and an increased risk with higher erythrocyte sedimentation rates in women.
Differential Diagnoses · Branch Retinal Vein Occlusion · Ocular Ischemic Syndrome
Workup
Laboratory Studies No laboratory studies are routinely indicated in the diagnosis of central retinal vein occlusion (CRVO). In older patients, laboratory testing should be directed toward identifying systemic vascular problems. In young patients, laboratory testing may be tailored depending upon individual findings, to include the following: · Complete blood cell (CBC) count · Glucose tolerance test · Lipid profile · Serum protein electrophoresis · Chemistry profile · Hematologic tests · Syphilis serology · In addition, thrombophilic screening, activated protein C resistance, lupus anticoagulant, anticardiolipin antibodies, protein C, protein S, and antithrombin III may be completed. Imaging Studies Color Doppler imaging is a noninvasive quantitative method of assessing the retrobulbar circulation. Detection of low venous velocities has been used to predict the onset of iris neovascularization. At present, this is performed as an investigational procedure in large facilities. [12] Optical coherence tomography (OCT) [13] scanning is a noninvasive, noncontact, transpupillary imaging technology that can image retinal structures in vivo with an axial resolution of 1-15 µm. OCT quantitatively measures the retinal thickness in micrometers in situ and in real time. OCT can detect even subtle macular edema in the presence of significant hemorrhages, which may not be evident on fluorescein angiography because of blockage from hemorrhage. OCT is used exclusively to monitor macular edema over time and the response with various treatment modalities. [13, 14] Other Tests Fluorescein angiography Fluorescein angiography is the most useful test for the evaluation of retinal capillary nonperfusion, posterior segment neovascularization, and macular edema. [2] Note the images below.
Fluorescein angiogram of a patient with nonischemic central retinal vein occlusion, showing staining of dilated tortuous veins with leakage into macula in a cystoid pattern.
Fluorescein angiogram of the same patient as in previous image, showing perifoveal capillary leakage in a cystoid pattern in late phases of angiogram.
Late phase of fluorescein angiograph of the same patient as in previous image, showing cystoid pattern of leakage from perifoveal dilated leaking capillary network. Fluorescein angiography is one of the tests used in the classification of CRVO. Areas of capillary nonperfusion are visualized as hypofluorescence, but hemorrhages can block fluorescence and give a similar picture. Therefore, in the early stages of the disease process, due to extensive hemorrhages, fluorescein angiography gives little information regarding the perfusion status of the retina. Once the hemorrhages clear, areas of capillary nonperfusion can be detected as hypofluorescence in the fluorescein angiography.
Various studies have reported different criteria for defining ischemic CRVO versus nonischemic CRVO based on the extent of capillary nonperfusion of the retina. The amount of retinal nonperfusion ranges from 10-30 disc areas. In addition, fluorescein angiography may show delayed arteriovenous transit, staining along the retinal veins, microaneurysms, arteriovenous collaterals, NVD, NVE, and dilated optic nerve head capillaries.
In a nonischemic central retinal vein obstruction, angiography may show minimal or absent retinal capillary nonperfusion, staining along the retinal veins, microaneurysms, and dilated optic nerve head capillaries. Resolved CRVO may be completely normal.
Macular edema may be detected as leakage from perifoveal capillaries (depicted in the image below), leakage from microaneurysms, or diffuse leakage on fluorescein angiography. If extensive edema is present, fluorescein angiography may show pooling of dye in large cystoid spaces. In addition, capillary nonperfusion around the fovea may indicate macular ischemia. If macular edema persists, pigmentary changes become evident.
Arteriovenous phase of fluorescein angiograph showing perifoveal capillary leakage in a patient with nonischemic central retinal vein occlusion. Optical coherence tomography angiography OCT angiography is an investigational method that generates high-resolution noninvasive angiograms that qualitatively illustrate most of clinically relevant findings in retinal venous occlusion. OCT angiography corresponds well with fluorescein angiography and, in many cases, provides more detailed anatomic and blood flow information. OCT angiography, in conjunction with standard spectral domain-OCT, is at least as effective as fluorescein angiography for evaluation and management of the macular complications of retinal venous occlusions. [15] Electroretinography Electroretinography (ERG) is another useful test to evaluate the functional status of the retina and to classify CRVO. [13, 16, 17] In ERG waveform, b-wave and a-wave are produced by the inner retina and the outer retina, respectively. In central retinal vein obstruction, perfusion of the inner retina is affected, so that the amplitude of the b-wave is decreased relative to the a-wave; the b-to-a ratio has been shown to be reduced. Some studies indicate that a b-to-a ratio of less than 1 suggests an ischemic central retinal vein obstruction. Histologic Findings
Not many histopathologic reports exist in the literature. A report of histologic sections of 29 eyes with central retinal vein obstruction showed a fresh or recanalized thrombus at or just posterior to the lamina cribrosa. Within the thrombi, a mild lymphocytic infiltration with prominent endothelial cells was seen. Loss of the inner retinal layers consistent with inner retinal ischemia also was seen. [18]
Treatment & Management Approach Considerations No known effective medical treatment is available for either the prevention of or the treatment of central retinal vein occlusion (CRVO). Identifying and treating any systemic medical problems to reduce further complications is important. Because the exact pathogenesis of the CRVO is not known, various medical modalities of treatment have been advocated by multiple authors with varying success in preventing complications and in preserving vision.
Macular edema is one of the prominent treatable causes of decreased visual acuity in patients with CRVO. The exact mechanism of macular edema is unclear, but multiple factors involved include increased venous pressure, elevated levels of VEGF, and deregulation of multiple inflammatory mediators leading to increased capillary permeability and leakage. Various treatment modalities have been used to counter different components of macular edema pathogenesis, with significant progress in stabilizing or improving visual acuity.
Advocated treatments are as follows: · Aspirin · Anti-inflammatory agents · Isovolemic hemodilution · Plasmapheresis · Systemic anticoagulation with warfarin, heparin, and alteplase · Fibrinolytic agents · Systemic corticosteroids · Local anticoagulation with intravitreal injection of alteplase · Intravitreal injection of ranibizumab · Intravitreal injection of aflibercept · Intravitreal injection of triamcinolone · Intravitreal injection of bevacizumab · Dexamethasone intravitreal implant
The Ophthalmic Technology Assessment Committee Retina/Vitreous panel of the American Academy of Ophthalmology evaluated available literature regarding efficacy of available pharmacotherapies in the treatment of macular edema due to CRVO. The panel reported that intravitreal anti-VEGF therapy is safe and effective over 2 years for macular edema and that delayed treatment is associated with worse visual outcomes. Intravitreal corticosteroid therapy yielded short-term efficacy but was associated with a higher frequency of adverse events. [19]
Medical Care Corticosteroid therapy Intraocular steroid injection has been shown to be effective in decreasing macular edema. Although the exact mechanism of action is unknown, steroids work by targeting various inflammatory pathways and decreasing expression of VEGF, reducing vascular permeability, stabilizing endothelial tight junctions, and decreasing macular edema.
Currently, triamcinolone acetonide and dexamethasone are the two steroid preparations used to treat macular edema associated with central retinal vein occlusion (CRVO).
|
Последнее изменение этой страницы: 2019-06-07; Просмотров: 192; Нарушение авторского права страницы