|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Cervical vago-sympathetic block
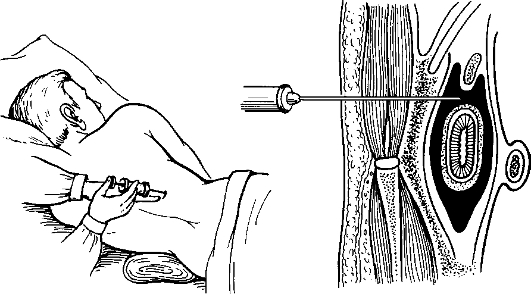
It is used to prevent pleurapneumonic shock in cases of injuries to the chest and as the basis for subsequent anaesthesia. The patient is placed supine with a fold under the neck, the head is turned to the opposite side with the hand on the blocking side drawn downwards. At the posterior side of the sternocleidomastoid muscle, in its mid-portion upper or lower its place of intersection with the jugular vein 0, 25% of novocain is injected to anaesthetise the skin. Using the left index finger push the muscle away anteriorly and medially together with the underlying vessels. Novocain (0, 25%) in a syringe with a long needle is injected through the skin, with some novocain pushed ahead and the needle advanced up and medially, using the anterior surface of the vertebra as the hallmark. Draw the syringe periodically to be sure you have not entered a blood vessel. 40-50 ml of 0, 25% of novocain are injected into each side if bilateral block is required. A successful block is achieved if Horner's sign (dilation of the pupil on the side of the intervention) is positive several minutes later. Paranephral lumbar block This method is used in blood transfusion shock, ileus (paralysis of the intestinal muscles), renal or hepatic colic. The patient is placed on the intact side with a folded sheet under the waist. The leg lying on the top is stretched, while the other one is flexed at the knee joint. The point of injection lies 1-1, 5 cm off the angle between the 12th rib and the latissimus dorsi muscle. After anaesthetising the skin insert a long needle perpendicularly to the body surface pushing along 0, 25% novocain. On crossing the lumbar fascia, which is felt as the overcoming of resistance, the needle arrives at the paranephric fat (fig. 12). If drawing the piston a little indicates the absence of blood, 60-80 ml of 0, 25% novocain are easily injected on each side. No solution trickling out after removing the syringe from the needle implies the needle has been in the right position. If some blood appears in the syringe, it should be withdrawn a little before injecting novocain. The latter spreads into the retroperitoneal fat engulfing the kidney, adrenal glands, solar plexus and coeliac nerves.
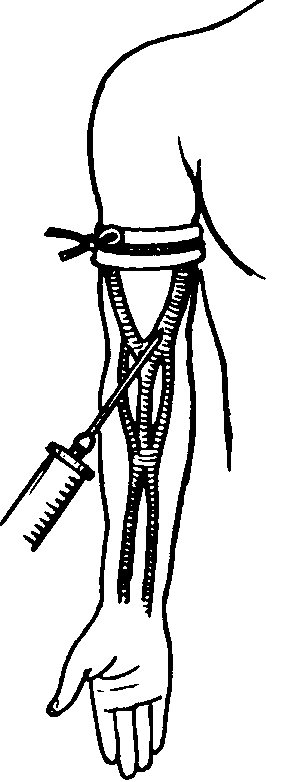
Fig. 12. Lumbar paranephric novocain block. Intravenous anaesthesia Intravenous anaesthesia is indicated for operations on the limbs (surgical debridement of wounds, manipulation of dislocations, repositioning of bone fragments, arthrotomy). The method is based on the local effect (by way of diffusion of the anaesthetic given intravenously) of anaesthetics on the nerve endings of the segment of the limb isolated from the main blood circulation by a tourniquet (fig. 13).
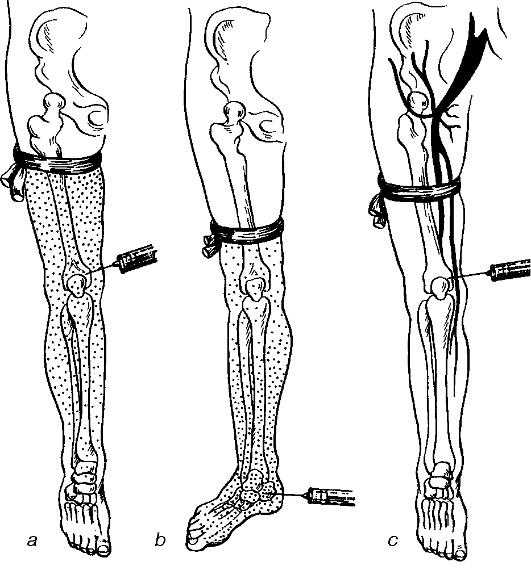
Fig. 13. Intravenous anaesthesia. Through venepuncture or venesection the anaesthetic is injected into the superficial veins of the forearm or elbow joint, or into the superficial veins of the leg. To enhance the venous blood flow, the limb is raised for 1-2 minutes and to stop arterial blood flow an elastic tourniquet is applied above the expected area of operation. During surgeries on the foot, leg or knee joint the tourniquet is applied on the lower third of the thigh; for operations on the fingers, hands, forearms or elbow joint - on the lower third of the arm. Instead of an elastic bandage for the tourniquet the cuff of a blood pressure apparatus can be used, air is pumped till the arterial blood flow is stopped. 150-200 or 200-250 ml of 0, 25% novocain are used for operations on the upper or lower limb, respectively. At the end of the operation the tourniquet or cuff is removed slowly to prevent the solution of novocain from fast penetration into the systemic circulation. Intraosseous anaesthesia This is also a form of intravenous local anaesthesia. The anaesthetic given into the bone enters the venous system of the limb from where it diffuses into the tissues (fig. 14). Intraosseous anaesthesia is used during operations on the limbs. The limb is isolated from the general blood flow by applying a tourniquet or the cuff of a tonometer. The anaesthetic is injected into the humeral condyles, olecranons and fingers, femoral condyles, tarsal bones or malleolae. The tourniquet is usually applied onto the arm, the lower third of the leg, the upper or lower third of the thigh. Immediately above the site of the puncture the skin and the underlying soft tissues as deeply as the periosteum are anaesthetised with 0, 25% novocain. A needle with mandrin used for bone puncture is pushed through the skin fatty layer and in a rolling manner is pushed into the cortical and spongy layers of the bone. 100-150 or 150-200 ml of 0, 25% novocain are used for surgeries on the upper and lower limbs or the thighs, respectively. After removal of the tourniquet toxic effect of the anaesthetic's resorption can sometimes occur (weakness, dizziness, hypotension, nausea and vomiting).
Fig. 14. Distribution of the anaesthetic following intraosseous anaesthesia. a - injecting the anaesthetic into the humeral condyle; b - injecting the anaesthetic into the ankle; c - inadequate application of the tourniquet results in the anaesthetic escaping into systemic circulation. To prevent the toxic effect of novocain, the patient is given 2 ml of caffeine solution subcutaneosly before removing the tourniquet which should be removed slowly. Potentiated local anaesthesia can be achieved by combining anaesthetics with neuroleptic drugs (e.g. droperidol) and general analgesics (e.g. phentanyl). In combined anaesthesia, which includes local anaesthesia and neuroleptic analgesia, local anaesthetic effect is enhanced by the positive action of the neuroleptic and the patient's psychic status. Neuroleptic analgesia and general anaesthesia are used to potentiate different kinds of local anaesthesia (infiltration, trunk block, spinal, epidural). With the aid of neuroleptic analgesia and general anaesthesia the dosage and therefore the toxic effect of local as well as narcotic agents can be reduced. Complications of local anaesthesia are related to allergic reactions of the anaesthetic drug or its overdose or that of epinephrine. Allergy to a local anaesthetic drug is manifested by skin rash, itching, Quincke's oedema, laryngoand bronchospasm. Antihistamines, glucocorticoids and spasmolytics are used to counteract the allergic reactions. Overdose of local anaesthetic substances occurs if large amounts of the drug are injected. Symptoms of overdose are anxiety, skin hyperaemic, fast pulse, hypertension, twitching or convulsions. In serious cases of intoxication the patient can develop collapse, respiratory or cardiac arrest or even coma. Mild cases of overdose can be managed with barbiturates, narcotic agents and oxygen therapy. Serious cases may require inotropic and vasopressor agents are given, and transfusion therapy with cardiopulmonary resuscitation may be necessary. Prevention of the complications includes a thorough interviewing the patient as to drug allergies and meticulous following the protocols of anaesthesia. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 104; Нарушение авторского права страницы