|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
HAEMOSTASIS (CONTROL OF HAEMORRHAGE)
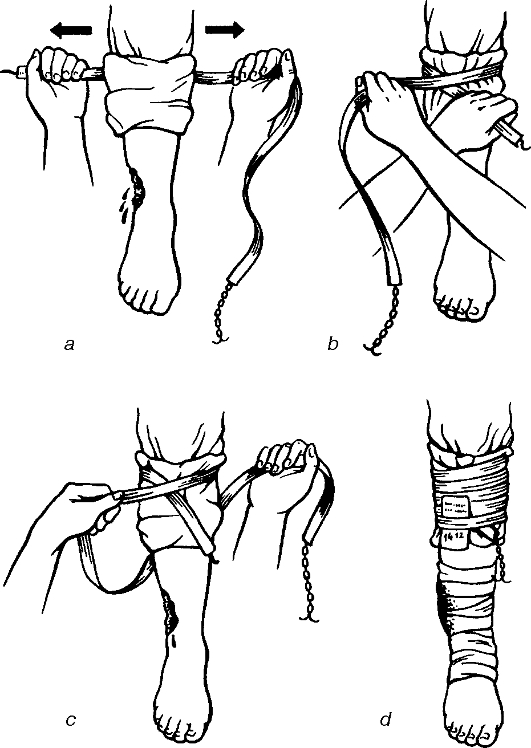
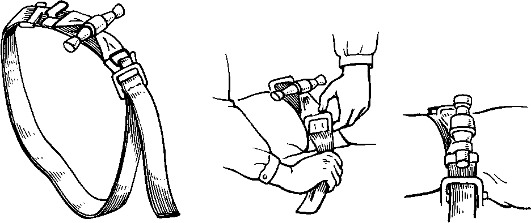
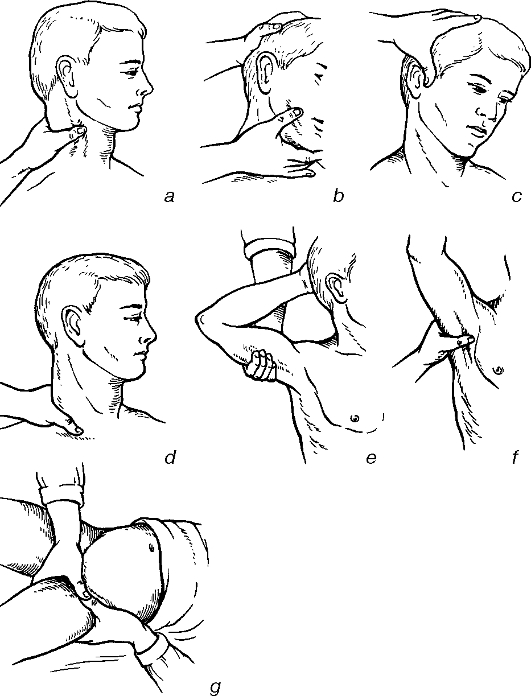
In majority of cases of bleeding from the arteries, veins or capillaries, haemostasis occurs spontaneously. Temporary methods of haemostasis. The most reliable way is the application of a tourniquet; however, it can only be used on the extremities (fig. 24, 25). In carotid arterial bleeding a tourniquet on the neck using a board or across the contra-lateral axilla is rarely applied. Instead, Cramer's splint is usually placed on the intact side of the neck to serve as a supporting frame. The tourniquet is applied to it and around some gauze pack that has been put on the bleeding vessel on the other side of the neck (fig. 26). If there is no splint at hand, the patient's intact hand is put on his/her head and bandaged.
Fig. 24. Application of the limb tourniquet: a - preparing the area for application; b - the start of the procedure; c - fixing the first round; d - the view after application.
Fig. 25. Application of the cervical «military» tourniquet.
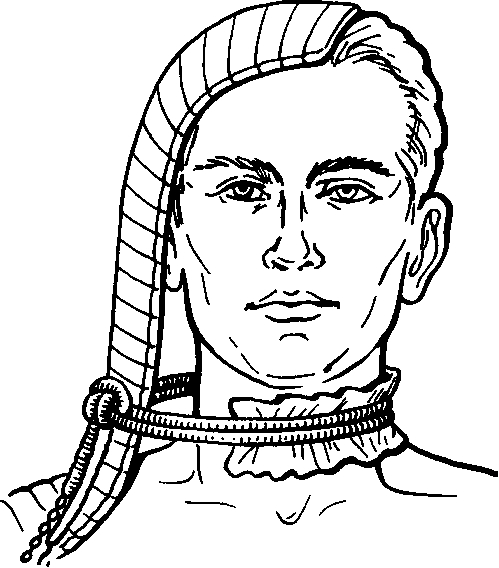
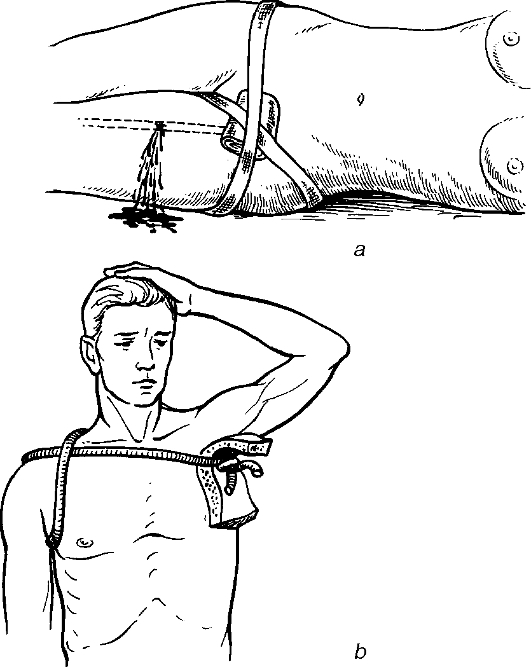
Fig. 26. Application of the facial tourniquet. Never apply a tourniquet to the abdominal aorta as this can cause damage to the abdominal organs. The tourniquets used to arrest bleeding are broad, flat, rubber bandages applied to the proximal parts of limbs which have been emptied of blood by the application of elastic bandages distoproximally (Esmarch's tourniquet) or 1, 5 m long tapes with metallic chains on one end and hooks on the other. In arterial bleeding or when massive bleeding is suspected the tourniquet will be applied above the injured site (fig. 27). First put a wet sheet or towel onto the area where the tourniquet is to be fixed, i.e. make a soft pad. The tourniquet should be applied firmly, for 2-3 rounds; the last one will be slightly loosed and fixed to the hooks. It is a must to write down the time when the tourniquet has been applied since keeping a tourniquet for more than 2 hours on the lower limb and for above 11/2 hours on the upper one can result in ischaemic necrosis. The disappearance of pulse on peripheral arteries, arrest of bleeding and a slightly pale discolouration of the skin below the tourniquet level suggest that it has been applied correctly. If the patient's transportation takes more than 11/2 hours, the tourniquet should periodically (every 10-15 minutes) be released until the reappearance of the arterial blood flow, before it is reapplied. At this point press on the bleeding vessel with the fingers in the wound or apply some instrument with a plug to the bleeding point. Reapply the tourniquet either somewhat below or above the original place. Subsequently, if necessary, the removal and reapplication of the tourniquet can be repeated (in winter time every 30 minutes, in summer each 50-60 minutes). Replace the tourniquet by a transportation splint, in cold periods the extremities being covered with warm clothes to prevent freezing. Transport the patient supine with analgesics having been given. Long and crude compression of tissues by a tourniquet can cause paresis and palsy of the limbs resulting both from traumatic damage to the nerves and ischaemic neuritis because of insufficient oxygen supply. Tissue hypoxia favours the proliferation of anaerobic infections, i.e. the species of bacteria able to survive without free oxygen. To prevent complications, stop bleeding by temporary application of an air-filled cuff to the proximal part of the limb. At this site the pressure applied must be higher than the arterial blood pressure. If the bleeding artery has been pressed on correctly, the haemorrhage can quickly be arrested; it is, however, difficult to keep pressing on a vessel for more than 15-20 minutes. Press on the artery at the sites where it lies superficially and around a bone (fig. 28, 29): • the carotid artery - the transverse process of the C6 vertebra;
Fig. 27. Application of the tourniquet in a damage to the femoral (a) and axillary (b) arteries.
Fig. 28. Topography of the arteries which can be pressed on for temporary bleeding control.
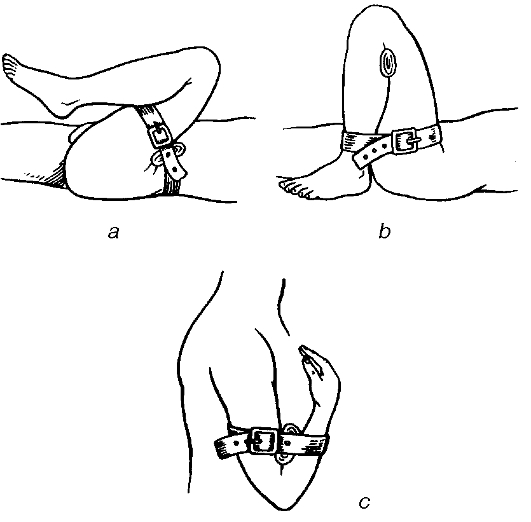
Fig. 29. Digital pressure on an artery to temporarily arrest the bleeding: a - the carotid artery; b - the sublingual artery; c - the temporal artery; d - the subclavian artery; e - the humeral artery; f - the axillary artery; g - the femoral artery. • the subclavian artery - the first rib; • the brachial artery - the internal surface of the humerus; • the femoral artery - the pubis. Unlike the carotid artery, the brachial and femoral ones can be pressed on easily. The subclavian artery is more difficult to press on as it is located behind the clavicle. Consequently, when the bleeding originates from the subclavian or axillary artery, fix the hand in a maximum extended backward position. Then press it on in between the clavicle and first rib. This is most important at the moment of tourniquet application or when changing it or during limb amputations. Flexion of the limb in a joint.. This method is effective provided that the limb can be flexed fully at the elbow joint and bandaged in that position to stop bleeding from the vessels of the forearm and the hand and at the knee joint to control haemorrhage from the vessels of the leg and foot. If the bleeding site of the femoral artery is too high for a tourniquet to be applied, the thigh can be fixed to the abdomen, with the knee and hip joints maximally bent (fig. 30). Wound package combined with application of a pressure bandage, immobilisation and raising the extremity is a suitable method of temporary haemostasis if the bleeding originates from veins or small arteries, soft tissues, the scalp, the elbow or knee joint. To achieve a tight package, the gauze should be tightly packed in the wound and pressure bandage applied over it. The tight packing of the knee fossa is contraindicated because this often leads to pedal gangrene. Pressure with load (e.g. a sand bag) or in combination with an ice pack (e.g. a bag with ice) is used for intratissue bleeding and prevention of postoperative haematoma. Digital compression of a vessel in a wound is indicated in emergency, occasionally during operations. For this, the surgeon will quickly put on sterile gloves or clean their hands with alcohol and iodine and press on the vessel or hold it inside the wound. If the bleeding vessel is located deeply inside (e.g. at the base of a limb, in the abdominal cavity, chest) and none of the methods of temporary haemostasis can be applied, the artery forceps or vessel clamps can be used. It is noteworthy that this can cause damage to some vital organs. Hence it is advisable to • control the bleeding by digital pressure; • dry the wound of blood; • apply the clamp on the bleeding vessel. Temporary bypass of a vessel is required to restore blood circulation in an injury to a major artery. A firm elastic tube is usually applied to both ends of the injured vessel and then fixed by ligatures. The temporary bypass can function for between several hours and several days, before the effective definitive haemostasis has been undertaken.
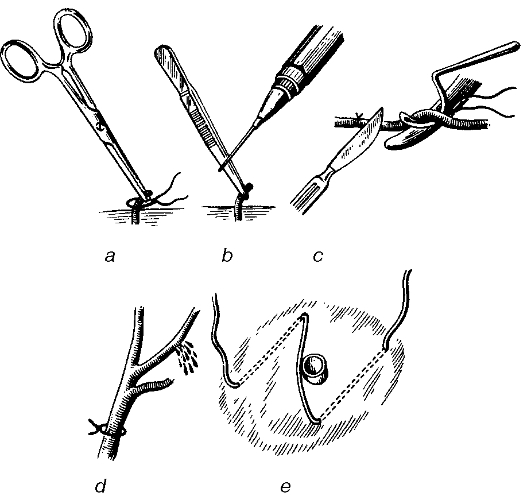
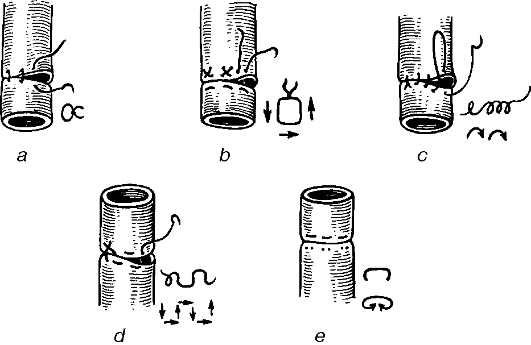
Fig. 30. Temporary control of femoral (a), popliteal (b), humeral and ulnar (c) arterial haemorrhage by means of maximal bending. DEFINITIVE HAEMOSTASIS The methods of definitive haemostasis divide into the four groups: 1) mechanical; 2) physical; 3) chemical and biological; 4) combined. Mechanical methods involve ligating the bleeding vessel inside the wound or somewhere along it. After the temporary arrest of bleeding has been achieved the definitive care will be provided. This involves surgical wound debridement, revision of the wound, and incision of the soft tissue along the vascular bundle. The vessel's central and peripheral ends are first identified; to pick these up and ligate the vessel artery forceps are used (fig. 31). Ligation of the vessel along its length is indicated when its ends cannot be identified in the wound. This precludes its ligation in the wound (e.g. injury to the internal and external carotid arteries). This is also the case in secondary bleeding when the eroded vessel is located in the midst of the inflammatory mass. This calls for identification, isolation and ligation of the vessel using the topographic landmarks, which, however, does not ensure the arrest of bleeding from the peripheral ends of the artery or its collaterals. When the surgeon fails to find the ends of the bleeder, they ligate the vessel together with the surrounding soft tissues. If it is not possible to ligate the vessel after its picking up with a clamp or forceps, the clamp can be left in the wound for 8 to 12 days (until the vessel has reliably thrombosed). Twisting of the bleeding vessel. To stop bleeding from small vessels, these can be picked up with a clamp and rotated. Wound packade. Bleeding from smaller wounds and injuries to small vessels can be arrested by packade. Dry swabs or those soaked in antiseptic solutions can be used. Anterior and posterior packades used to stop the nasal bleeding can serve as a typical example. Bleeding from the vessels that are difficult to ligate can be stopped using silver clamps (i.e. vascular clamping). For primary arrest of bleeding from the hollow viscus; part of the organ (e.g. stomach resection in bleeding gastric ulcer) or a whole organ (e.g. splenectomy in ruptured spleen) has to be resected. Special sutures may occasionally be applied (e.g. at the edge of the liver affected). To stop bleeding from the lung, gastrointestinal tract and cerebral vessels a special method of artificial vascular embolism has been recently implemented; this involves the use of lysing (e.g. gelatin, muscle homogenate) or non-lysing (e.g. silicon, polysterol) substances. Vascular sutures. There exist both manual and mechanical vascular sutures. Suturing a vessel is recommended whenever restoration of the patency of major vessels is necessary. Circular vascular sutures are placed manually using atraumatic needles (fig. 32). Ideally, an «end-to-end» connection is performed. Vascular sutures should be very compact and airtight and meet the following requirements:
Fig. 31. Definitive methods of haemorrhage arrest. a - vascular ligation; b - electrocoagulation; c - vascular ligation using transection; d- vascular ligation in continuity; e - mediate ligation.
Fig. 32. Vascular sutures. a - interrupted (Carrel-type); b - mattress; c - blanket; d - continuous mattress; e - mechanical. 1) a lack of strictures or bumps (not to impede the blood flow); 2) minimum threads appearing in the lumen. Circular vascular sutures can be made using tantalum staples, Donetski's ring. Mechanical sutures are perfect enough not to obstruct the vascular lumen. Lateral vascular sutures are placed when the vessels are injured adjacently. On suturing, the vessel can be strengthened with the muscle and fascia. A large tissue defect resulting from the injury or surgery (e.g. following the excision of a tumour) can be covered with a patch from biological materials (e.g. fasciae, aponeuroses, muscles and venous walls). An «auto-vein» (the superficial veins of the thigh or forearm) is most commonly used. In vascular surgery autoand allotransplants of arteries and veins are used for grafting (e.g. heterografts or xenotransplants, which are made of synthetic compounds). Performing an «end-to-end» anastomosis or suturing the graft ensures reconstruction. Physical methods. Thermal means of haemostasis is based on the fact that on exposure to high or cold temperatures proteins coagulate inducing a clot formation cold can cause vascular spasm. This is of great importance for bleeding arrest during operation. In diffuse bleeding from a bone a piece of gauze soaked in hot normal saline is applied. The application of ice packs in cases of subcutaneous haematoma or swallowing of ice cubes in cases of gastric bleeding is widely used in surgery. Surgical diathermy involves the passage of high frequency electric current by knife or button electrode to generate heat in the tissues for the coagulation of bleeding vessels. It is mainly used to control bleeding from subcutaneous and muscles' vessels as well as from minor vessels of the brain. The surgical diathermy may be applied provided that the wound is dry, and the voltage of the current is not high enough to cause tissue burn since it can itself cause bleeding. Laser (focused beam of electronic rays) is used in patients with peptic ulcer-associated upper GIT bleeding, haemophiliacs and in oncologic operations. Cryosurgery is the local application of cold, mostly in tumours of the organs with intense blood supply (e.g. the brain, liver, kidney). Local freezing of tissues is safe to the areas surrounding those exposed to cryonecrosis. Chemical and biological methods. Haemostatics may be of a resorptive or topical action. Resorption occurs when the substance enters the circulation, while topical effect is visible on the direct application to the bleeding tissue. Haemostatics with resorptive action are widely used for internal bleedings. Direct blood transfusion is the most effective. In addition, transfusion of small amounts (100-150 ml) of freshly frozen blood, plasma, platelet mass, fibrinogen, prothrombin complex, anti-haemophilic globulin, cryoprecipitate is also recommended. These agents are indicated for congenital or acquired deficiency of blood coagulating factors as is the case in pernicious anaemia, leukaemia, haemorrhagic disorders etc. Currently, inhibitors of fibrinolysis have been widely used to decrease the blood fibrinolytic activity. Bleeding associated with an increase in the blood fibrinolytic activity is encountered during operations on the lung, heart, prostate, in liver cirrhosis, sepsis and following transfusion of large amounts of blood. Biologic anti-fibrinolytic substances include contrycal, trasylol (aprotinin), while aminocapronic acid and ambenum are synthesised. Dicynone and etamsylate enhance the formation of thromboplastin, normalise vascular permeability and improve microcirculation.Rutin, ascorbic acid and carbazochrome are used to normalise the permeability of vascular walls. Vicasol, a synthetic water-soluble analogue of vitamin K, is applicable for haemorrhage associated with a deficit of prothrombin (e.g. acute hepatitis and mechanical jaundice, parenchymal and capillary bleeding following injuries and surgical manipulations, gastrointestinal and nasal bleeding, haemorrhoids). Conversion of prothrombin to thrombin requires a slight amount of calcium ions that are available in the blood. Therefore, the use of calcium as a haemostatic substance is justified only in massive transfusion of citrated blood, since on reaction with calcium citrate ions tend to lose their anticoagulative properties. Topical haemostatics. In parenchymal bleeding resulting from a liver rupture specific biologic packs (a muscle or the omentum as a free flap or a peduncular flap, i.e. a flap on a peduncle) are used. Quite effective is the use of fibrin sponge, biological antiseptic pack, haemostatic and gelatin sponges. Haemostatic and gelatin sponges, biological antiseptic packs are used to arrest bleeding from bones, muscles, parenchyma organs, capillaries, as well as for the packade in bleeding from the sinuses of the dura matter. Thrombin (a substance obtained from the plasma of donor blood) is effective in capillary and parenchymal bleedings as it influences the conversion of fibrinogen into fibrin. Prior to its use it will be dissolved in normal saline to soak sterile gauzes or the haemostatic sponge and then applied to the bleeding surface. The use of thrombin is contrain-dicated in bleeding from major vessels, since it can induce the fatal generalised thrombosis. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 63; Нарушение авторского права страницы