|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Methods and types of products for transfusion
In anaemia, leucopenia, thrombocytopenia and clotting disorders when particular blood components are deficient, transfusion of whole blood is not justified. The whole blood therapeutic effects in such cases are therefore low whilst the waste of blood is unreasonably high. Instead, concentrated blood components (e.g. red blood cell or leucocyte mass, plasma, albumin) are to be used. Patients with haemophilia, for example, will only need transfusion of factor VIII. Again, instead of giving litres of whole blood, the therapeutic effect can be achieved by giving only a few millilitres of antihaemophilic globulin. In hypoand afibrinoginaemia, up to 10 l of whole blood may be needed to compensate for the deficit in fibrinogen, whereas only 10-12 g of the blood product of fibrinogen may suffice. Besides, transfusion of whole blood can lead to sensitisation of the patient, the formation of antibodies to blood cells (leucocytes, platelets) or plasma proteins, which can cause serious complications during subsequent blood transfusions or pregnancies. Transfusion of whole blood is indicated in acute haemorrhage with a dramatic decrease in the circulating blood volume, in exchange blood transfusions, in heart-lung bypass during open heart surgeries. It is recommended that the product for transfusion contain the components of blood that the patient needs most of all (tab. 3). Examination of preserved blood and its components before transfusion. The blood to be transfused has to be examined for viability (fig. 37, colour inset): the wholeness of the package, expiring date and possible violations of storage (frozen or otherwise overheated). The best blood to transfuse is the one that has not been stored for more than 5-7 days, since a longer storage period may result in biochemical and morphological changes which reduce the positive properties of blood. Macroscopically, blood should have three layers. The red layer of red blood cells is located at the base followed by a thin layer of leucocytes and the top transparent yellowish layer of plasma. Signs which show that blood is not fit for transfusion are as follows: red or pink discoloration of plasma (haemolysis), the presence of flakes, cloudiness, the presence of a film on the surface (signs of contamination), the presence of clots (clotted blood). In emergency blood transfusions some of the blood is put in a glass tube and centrifuged. Pink discoloration of plasma indicates haemolysis. To transfuse frozen blood components the package is quickly warmed to 38 °C, the cryostabiliser (glycerin for red blood cells and dimethyl sulphoxide for leucocytes and platelets) is then washed off red blood cells. Cross-matching (i.e. checking) the blood groups of the donor and recipient's blood. Although the data from the patient's case history may coincide with those on the the labels on the blood bag, it is necessary to repeat typing the patient's blood group of the patient that of the blood to be transfused immediately before the procedure. It is the physician who will perform transfusion is responsible for checking. In emergency transfusion, apart from checking the blood group by the ABO system, Rh is checked using the express method. The grouping is done according to the stipulated rules and regulations and the results are observed not only by the doctor performing the transfusion but also by other doctors. Testing for compatibility. To check for individual compatibility 3-5 ml of blood is taken from the patient's vein, this is centrifuged or allowed to stand. One big drop of the serum is then put on a plate or flat surface. A drop of donor blood is placed nearby at the ratio of 5: 1 - 10: 1, mixed together by a glass rod or the slide edge and observed for 5 minutes, after which a drop of normal saline is added and the result determined by the presence or absence of agglutination. The absence of agglutination indicates that the blood groups of the patient and the donor are compatible, and the presence of it means incompatibility (fig. 38, colour inset). This checking for compatibility is to be performed on each bag of blood that is to be transfused. Checking for compatibility of the Rh is done in the case of unfavourable transfusion history (previous post-transfusion reactions, Rh conflict pregnancies, miscarriages), in critical conditions when it is not possible to recheck the patients Rh, and in a case when the patient with unknown Rh has to receive Rh positive blood. Blood is taken from the vein like in checking individual compatibility for grouping, centrifuged, a drop is put into the Petri dish and a smaller drop (3-5 times smaller) of the donor blood is added, mixed together, covered and allowed to float on a water bath at 42-45 °C for 10 minutes. Table 3. Indications of transfusion solutions
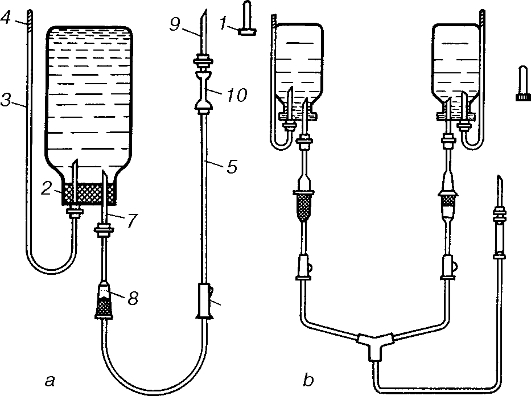
The checking is better done in light using a magnifying glass. The absence of agglutination allows for the transfusion of blood in that package. The presence of agglutination indicates that the patient's blood is Rh negative, and contains anti-rhesus antibodies (fig. 39, colour inset). Such a patient can only be transfused with Rh negative blood. Compatibility test for the Rh has to be done on each donor pack that is to be transfused. If true agglutination is encountered in the process of the ABO system and Rh tests, the specific donors have to be searched for the particular patient through the blood bank. Assuming the patient's condition is critical and urgent blood transfusion is needed, a search is done through the available stock without waiting for an answer from the blood bank. Blood is chosen from the same group and Rh. Blood from each pack is tested with the serum of the patient according to the ABO system and the Rh for compatibility. If agglutination does not occur, that blood can be transfused starting with the biological test. In case the tests from all the existing blood in stock with the same groupand Rh give positive reactions of agglutination, none of them can be transfused and the patient will have to wait for an individual donor to be found through the blood bank. If such blood is received through the blood bank, it still has to be grouped and cross-matched again for the ABO system and Rh as well as for individual compatibility. It is only when the patient's blood is of the same group and Rh with the donor blood and there is no sign of agglutination in the compatibility tests for the ABO system and Rh that the blood can be transfused always starting with the biological test. Preparation for transfusion. Blood is transfused through a disposable plastic system with nylon filter preventing blood clots from entering the blood stream (fig. 40). The system consists of a short tube with a needle and filter for allowing air into the bottle, a long tube for the infusion of blood with a needle at each end - one to put into the bottle and the other to puncture the patient's vein. The system is fitted with a dropper, nylon filter and a plastic clamp to regulate the rate of infusion. They are produced in sterile forms packed into polyethylene bag which should be opened only immediately before use. Transfusion sets that can be used for several times are not advisable since they are not equipped with micro filters. However, when needed, a non-pyrogenic tube has to be used, a glass dropper that controls the rate of flow is mounted onto it, and a glass tube attached towards the outlet controls the complete exit of air out of the tube while filling with blood. To attach the system to the bottle, two special needles - a long and short ones which are inserted through the rubber cork of the bottle. The longer needle is inserted as deep as the bottom of the bottle, and it is through it that air escapes during the time of transfusion, the shorter needle is attached to the plastic tube for transfusion, onto which the plastic clamp is fitted; the bottle is turned upside down and hung on the drip stand. The system is subsequently filled with blood after all the air has been expelled from it.
Fig. 40. The blood and fluid infusion system. (a) the mounted system: 1 - needle cover; 2 - bottle filled with blood; 3 - air-way tube; 4 - air-filter; 5 - transfusion tube; 6 - clamp for regulating the blood flow rate; 7 - needle for blood flow from the bottle; 8 - dropper filter; 9 - needle for venepuncture; 10 - joining tube; (b) multi-bottle blood and fluid infusion system. Mounting the system for transfusion one should abide by the following regulation: transfuse blood from the bottle in which it has been prepared and stored. When transfused from a plastic bag, blood is first mixed by shaking the bag, a clamp is put on the central outlet tube, alcohol or 10% iodine is used to cleanse the tube which is cut at about 1-1, 5 cm below the clamp. The safety cap of the system is removed and attached to the system by way of attaching the tube end of the bag to the cannula of the system. The bag of blood is hung upside down onto the drip stand, the system with the dropper is raised and turned so that the filter in the dropper is situated on the upper part. The clamp is removed from the tube; the dropper is half filled with blood before the clamp is reapplied. The system is put back to its original position with the filter downwards and must be filled with blood. The clamp is removed and that part below the filter is filled with blood until all the air in it is evacuated and blood drops start coming out of the needle. A few drops of blood are let onto the plate for onward control determination of the grouping, Rh of the donor blood and compatibility. The system is checked through observation to make sure there are no air bubbles inside. The system is now ready for use. The rate of infusion is regulated with the clamp. When it is necessary to change an empty bag with a new one, the system is closed with the clamp, a few forceps are used to clamp the tube, the old bag is removed and a new one attached. Blood transfusion using the standard bottle. The top of aluminium cap is removed, the adjacent rubber cork is then cleansed with alcohol or iodine tincture and punctured with two needles. A short tube is attached to one of the needles for air passage, the end of which placed above the bottom of the bottle, and to the other needle is attached the disposable system with the bottle hung upside down on the drip stand. The system is filled with blood as mentioned above. After mounting the system and determination of the grouping and Rh as well as the compatibility tests blood transfusion can be started. The system is attached to a needle that has previously been inserted into the vein with some solution for infusion already running. The test for biological compatibility. Transfusion of blood or its components (red blood cell mass, red blood cell suspension, plasma) has to be preceded by the biological test for compatibility. To perform this test, the first 15-20 ml of blood are allowed to flow fast; the infusion is stopped and the patient's response and condition are observed (behaviour, skin colour, pulse and breath rates). Tachycardia, dyspnoea, facial hyperaemia and hypotension all suggest incompatibility of the donor's blood with that of the recipient. In the absence of signs of incompatibility the test is repeated twice, and if there are still no reactions the blood transfusion is continued. During the triple biological test the needle can be thrombosed when the infusion is halted. To prevent this when infusion is supposed to have been halted, it can be allowed to drop at a very slow rate or if blood substitutes are to be given with the blood, they can be given in those intervals. Supervision of blood transfusion. The rate of flow is regulated with a special clamp. Blood is to be given in drops at a rate of 50-60 drops/minute. If fast flow of blood is needed, the clamp is fully opened, or a Richardson's cylinder can be attached to pump in air into the bottle (transfusion under pressure). The patient has to be closely observed throughout the whole period of transfusion, so that in case there are any complications or reactions they can be noticed, and transfusion stopped early enough to start therapeutic measures. If the lumen of needle is blocked by a thrombus, it is not advisable to use any solutions or the mandrin as it may push the thrombus further into the patient's vein. In such a case it is advisable to clamp the system, disconnect it from the needle, remove the thrombus from the vein and apply a pressure bandage; a new needle is then used to puncture a new vein to continue with the transfusion. It is allowed to mix sterile intact blood substitutes that are in standard packages with the blood in the process of blood transfusion. Transfusion is stopped when about 20 ml of blood are left in the bottle, ampoule or plastic bag. The needle is removed and a sterile dressing is bandaged on the puncture site. The blood left in the bottle is stored under sterile conditions in the refrigerator at 4 °C for 48 hours. In case the patient develops a reaction later this left over blood can then be used to investigate the cause of the complication (checking for bacterial contamination, blood group and Rh cross-matching, retesting for compatibility of the donor blood with the patient's blood). Recording blood transfusion. Every blood transfusion must be recorded into a special book meant for this purpose as well as into the patient's case history. Such information as the amount of blood given, the data written on the given blood pack, the result of the compatibility test and reactions or complications, if any, are to be noted. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Последнее изменение этой страницы: 2019-06-08; Просмотров: 69; Нарушение авторского права страницы