|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
ARTERIAL OCCLUSION (ACUTE AND CHRONIC ARTERIAL INSUFFICIENCY)
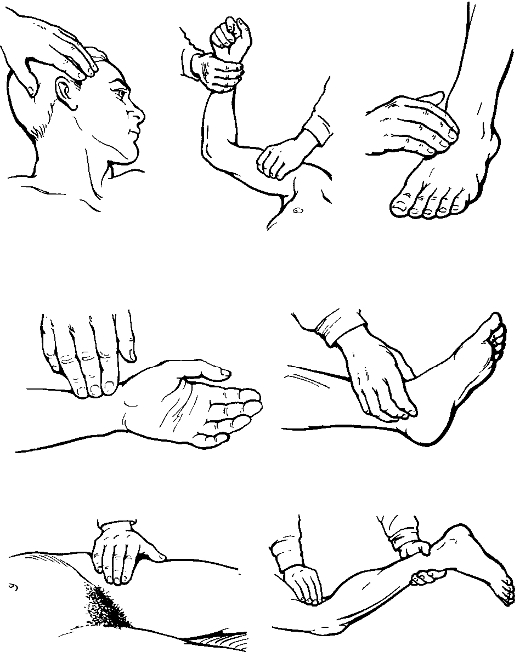
Examining the patient with arterial diseases the surgeon has to consider a number of peculiarities: 1. The examination must occur in a warm room. 2. It is required that the symmetrical sites of the limbs be inspected. Skin colour is compared on both limbs. Pale or violet-bluish discolouration acquired on moving the limb from the horizontal position to the vertical one strongly suggests deficient circulation. The skin is usually dry and scaly, and the nails are deformed, thickened and brittle; a loss of hair and muscle atrophy may also be observed. The feeling of the arteries shows a weak or absent pulse. On the lower limb the pulse is to be felt on the femoral artery (below the middle of the Poupart's ligament), popliteal artery (in the popliteal fossa with the leg flexed in the knee joint and the muscles maximally relaxed), dorsalis pedis artery (between the first and second metatarsal bones) and tibialis posterior artery (behind the medial malleolus). Pulsation on the upper limb will be evaluated on the subclavian, humeral and radial arteries (fig. 131). To assess the severity of arterial circulatory disorder special tests are performed. Oppel test. Have the patient lie supine with his/ her leg raised at an angle of 45°. The appearance of paleness on the sole (the plantar ischaemic sign) serves as the evidence of arterial circulation insufficiency.
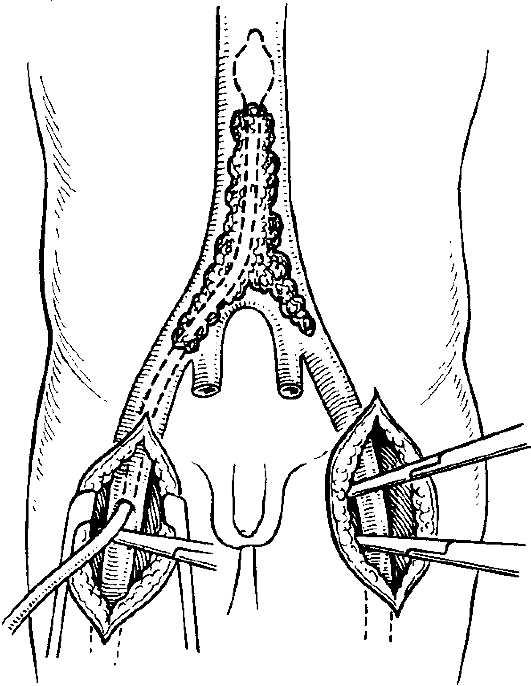
Fig. 131. Feeling the peripheral artery pulse. Samuel's test. Have the patient lie in the position as described above and do 20 to 30 flexions in the ankle joint. The appearance of paleness on the sole is also a sign of arterial circulation insufficiency. Moshkovich's test. Have the patient lie supine raise his/her leg and apply a tourniquet for 5 minutes. The period needed for the skin to regain hyperaemia following the removal of the tourniquet is normally 5 to 30 seconds whereas that in arterial occlusion is as long as 3 to 5 minutes. The above-mentioned tests can only be diagnostic at initial, or compensated, stages of the disease. If intermittent claudication appears, the diagnosis is easy to make (the suband decompensation stages of circulatory failures). Special methods are used to assess the severity of circulatory disorders, monitor pathologic progression and the efficacy of therapy. These are primarily as follows: 1. Thermometry, the technique of measuring skin temperature at symmetrical limb areas using an electric thermometer. A reduction in temperature by 0, 5-0, 7 °C strongly suggests deficiency in the blood flow. 2. Oscillography, recording oscillations produced by changes in electrical potentials caused by vibrations of an artery. A decrease in vibration amplitude indicates deficient circulation. 3. Impedance rheovasography, the technique to register the resistance produced by pulsating limb arteries as a result of their filling. In health, the rheographical index is as high as 0.8-1.0; its reduction being evident of deficiency in the arterial circulation. 4. Doppler ultrasound, the method of listening to the arterial blood flow with the velocity detector (Doppler probe) to recognise arterial occlusion or stenosis. 5. Capillaroscopy, microscopical examination of the capillary vessels of the skin or nail beds. In occlusive arterial diseases the capillaries become convoluted, winding and constricted. 6. Arteriography, the visualisation of arteries by means of X-rays after injection of radio-opaque material. In obliterating atherosclerosis, the vessels with the «eaten up» internal contours, as well as areas of the constricted, or occluded, lumen are seen. In endarteritis, the arterial lumina are markedly narrowed, often over wide areas. Thrombosis/thromboembolism cause obstruction of the artery. ACUTE ARTERIAL OCCLUSION Acute arterial occlusion is the condition that results from the sudden arrest of the blood flow in an artery and is the commonest cause of gangrene. The factors that contribute to arterial occlusion include trauma, the excessive pressure from a tourniquet, intra-operative ligation of the artery, thromboembolism (i.e. the obstruction of a vessel, mainly by thrombus and occasionally by air, fat). Arterial embolism results in ischaemia of the limb, the severity of which depends on the size of the thrombosed vessel, the level of obstruction, the capacity of the collateral circulation as well as the duration of the problem (the time lag between the moment of occlusion and the reporting time). In thromboembolism of a major artery, the sign of acute organ ischaemia (e.g. the limb) is observed. Thromboembolism causes the following pathogenic changes: • obstruction of a main vessel; • acute distension of the vessel above the area of obstruction; • reflex spasm of all the arterial network of the limb - the obstructed vessel, its branches and collaterals beneath the area of obstruction; • formation of a sequel thrombus beneath the area of obstruction because of a decrease in blood flow and defects of blood coagulation and anti-coagulation systems. To verify the diagnosis and identify of the level of occlusion special investigations are applied: cutaneous thermometry, oscillography, rheography and angiography. According to V. Saveliev, the clinical course of thromboembolism of the major vessels divides into three stages: • stage 1 - ischaemia causing functional disorders. This lasts a few first hours. The clinical picture includes (1) acute pain in the limb affected, (2) pale and cool skin, (3) absent pulse on the peripheral arteries. It is noteworthy that pain and touch senses usually remain intact, active joint motions are slightly limited. The restoration of blood supply to the limb at this stage leads to a full functional recovery; • stage 2 - structural changes - includes such signs as absent pain and touch sensations, markedly limited active and passive joint movements, muscular oedema and contractures, bluish discolouration of the skin. This stage lasts for 12 to 24 hours. The restoration of blood supply within the above-mentioned period, can save the limb although its functions are, as a rule, either partially or fully lost; • stage 3 - necrosis - is characterised by the development of gangrene. It follows within 24 to 48 hours after embolisation. At this stage, due to gangrene virtually all forms of sense and movement will be lost, while resume of the blood flow in the vessel can occasionally reduce the level of the demarcation line, hence the level of amputation. The staging of ischaemia helps choose the therapeutic modality: • stages 1 and 2 require radical treatment - restoration of the artery's patency (i.e. restoration of the blood flow); • stage 3 precludes the aforementioned therapy as the necrosis of an extremity is a life-threatening condition and thus calls for urgent options, of these the amputation of the limb affected being the mainstay. The clinical features of the disease, leg pain particularly, may readily be identified the moment embolisation has occurred. The severe ischaemic pain, which results not only from occlusion but also from the reflex spasm of collateral vessels, is of sudden onset and of persistent duration. Occasionally, it can produce shock. The pain is mostly often located at the distal parts of the limb; it sometimes appears at the area of occlusion and spreads distally later on. Alternatively, the patient may present with numbness sensation, paraesthesia (tingling), while coolness to touch and pain come on thereafter. This suggests that the incomplete occlusion of the artery by an embolus precedes the complete one due to secondary thrombosis that causes limb ischaemia. The incidence of the subacute course of thromboembolism of a major artery is as high as ten percent. The patients with arterial thromboembolism are usually those with serious cardiac disease, which accounts for the severity of their condition. Physical examination yields helpful clinical signs as follows: 1. Vital signs: • increased pulse rate; • low blood pressure (a sign of impending shock); • labial and mucosal cyanosis; • fast breathing. 2. Skin: • a change in the skin colour, which becomes cyanotic, pale or even white with bluish patches («the marble skin») that resemble those of the cadaver; • coolness to touch is more pronounced at the peripheral areas; skin temperature is reduced by 2-3 °C as compared to that of the intact side; • both pain and touch sensations checked with a needle are diminished. The inability of the patient with their eyes closed to distinguish between being pricked by a sharp object and touched by a blunt one indicates the loss of both pain and touch sensations. This suggests irreversible damage to the tissues as the circulation in the limb fails to maintain the viability of tissues. 3. Pulses: • absent lower limb pulse is a typical sign. 4. Neurologic signs. It should be emphasised that neurological signs (numbness sensation and paraesthesia with subsequent loss of all kinds of sensation) become visible very fast. The pain can shortly be followed by motor deficit of various degrees (finger and toe paralyses). The combination of pulselessness with paraes-thesias, acute pain, pallor and palsy are therefore diagnostic of acute arterial ischaemia. If measures are not taken to restore circulation, the signs of acute ischaemia progress and gangrene, which is usually dry ensues. Treatment. The first aid in arterial thromboembolism includes: (I) analgesia and cardiac medications; (II) transport immobilisation of the limb either by a standard or an improvised splint; (III) application of ice packs to the affected limb; (IV) immediate transportation of the patient to the surgical unit. The management of the patient with arterial thromboembolism must be individualised depending on (1) the location of the embolus; (2) the stage of disease and (3) its duration. The preoperative treatment should start with conservative measures. Failure of ischaemia to subside and that of pain to relieve and touch sensations to recover within 11/2-2 hours of the therapy is an indication for surgery. The conservative treatment is applicable: (I) at the initial stages of the disease (i.e. within 6 hours from its onset of disease); (II) in critically-ill patients; (III) in embolism of small arteries (i.e. those of the foreleg and forearm); (IV) in obscure clinical picture; (V) as a method additional to surgery. It involves the following: 1. anticoagulation therapy (heparin, indirect anticoagulants) and fibrinolytic agents (streptokinase, streptodecase, urokinase) to prevent formation of clots and lyse the the preformed ones; 2. antispasmodic therapy to eliminate the vascular spasm (vasodilators, novocain block, papaverin, carbacholin); 3. improvement of collateral circulation (Bernard's current; vacuum apparatus applied to the limb). Surgical treatment implies radical operations (i.e. embolectomy (fig. 132), arterioplasty and vascular shunting) to restore the patency of arteries, whereas palliative ones are performed to improve the collateral circulation without restoring the patency of the main vessel (e.g. sympathectomy). The gangrenescent limb is subject to amputation.
Fig. 132. Embolectomy using a balloon catheter. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 46; Нарушение авторского права страницы