|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
SUPPURATIVE DISEASES (PURULENT INFECTIONS) OF SEROUS CAVITIES
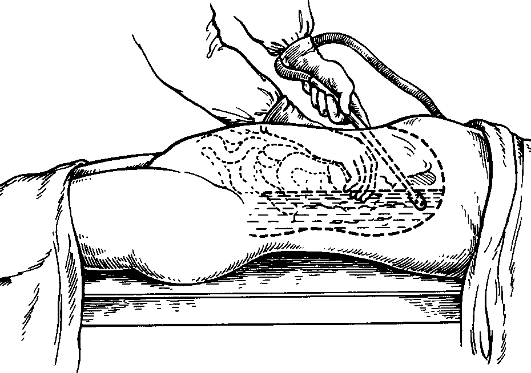
Purulent (suppurative) peritonitis - this is the inflammation of the parietal and visceral peritoneal layers accompanied by local changes and intoxication. Classification 1. According to the extent of spread of the disease: a) localized peritonitis: circumscribed (enclosed), unlimited (not enclosed); b) generalized peritonitis: diffuse; c) general (total) peritonitis. 2. According to the stage (phase) of development: a) the reactive stage (1st 24 hrs); b) toxic phase (24 to 72 hrs); c) the phase of polyorganic failure (after 72 hrs). The main processes that determine the clinical picture of suppurative peritonitis are the inflammation of peritoneum and paresis of the intestines. The inflammation of peritoneum is accompanied by profuse exudation into the peritoneal cavity. The exudate is initially serous, then seropurulent and then purulent. When fibrin is present the exudate becomes purulofibrinous, and in the case of ichorous tissue disintegration, it becomes ichorous. Excessive exudation causes the escape of proteins from the blood flow into the peritoneal cavity, primarily albumins, then water and electrolytes. The amount of exudates accumulated into the peritoneal cavity can reach several liters with protein content of 5% or more. Protein loss (including the exudates, vomitus etc.) varies between 50-250 gm a day, and in cases of continuous perfusion of the abdominal cavity can reach up to 400 gm a day. The protein content of the blood sharply decreases, the patient develops disproteinemia. Large amounts of protein loss during peritonitis compromise the nutritional status of the organism. All this leads to the mobilization and depletion of the energy reserve (glycogen, fat deposits) and disorders in all types of metabolic activities - protein, carbohydrates, fat, and water-electrolyte. The accumulation of fluid in the abdominal cavity as well as its loss through vomitus leads initially to cellular dehydration and later to water deficit both intracellular and in the extracellular space. Water is lost together with large amounts of salts, the deficiency in water is augmented by electrolyte deficiency, especially potassium. The acid-base imbalance is characterized by a shift in the direction of metabolic acidosis or alkalosis and closely linked to the imbalance of electrolyte metabolism, functions of the respiratory, cardiac and renal systems. A special feature of peritonitis is the spread of infection and the intensive absorption by the peritoneum of toxic products - bacterial toxins, and products of tissue disintegration. The development of peritonitis is accompanied by the paralysis of the gastrointestinal tract. The intestinal lumen is filled with contents that undergo decomposition and contain large amounts of microorganisms. The absorption from the intestines of bacterial toxins, toxic products of putrefaction and fermentation worsen the already serious intoxication caused by the purulent inflammation of the peritoneum. Hemodynamic disorders figure significantly in the complex of pathophysiological reactions that occur in purulent peritonitis. Common to them is the inconsistency between the vascular space volume and the amount of blood in circulation, which is associated with a decrease in the blood pressure, disorders in the microcirculation, cardiac function and the blood supply to the organs. The changesin the rheologic properties of blood are instrumental in the development of microcirculatory disorders. Purulent peritonitis is normally a secondary disease caused by the spread of infection from an organ in the abdominal cavity onto the visceral and parietal peritoneum. Peritonitis may be attributed to one of the following causes: acute appendicitis, acute cholecystitis, perforated stomach and duodenal ulcers, intestinal obstructions, acute pancreatitis, trauma to the abdominal organs and pelvic inflammatory diseases (the internal female genital organs). Peritonitis can also result from surgery (postoperative peritonitis), when contamination of the peritoneum occurs accidentally during operation or as a result of the breakdown of anastomosis after the operation. Purulent peritonitis is classified according to the spread and phase of the disease process. In clinical practice after the diagnosis of peritonitis has been established it is imperative to identify the source of infection, the extent of its spread and the disease stage. Localized unlimited (not enclosed) peritonitis according to the extent of spread occupies up to 2 out of the 9 anatomic areas of the peritoneal covering. The process can spread along the peritoneum involving new areas in the inflammation. Localized circumscribed peritonitis is characterized by formation of inflammatory infiltrate, adhesions, scars that prevent the infection from spreading to other areas of the peritoneal cavity, resulting in the formation of intraabdominal abscesses. When the inflammatory process involves more than 2 of the anatomical areas but less than 5 (more than one but less than two floors of the abdominal cavity) without the signs of limitation (encapsulation), such peritonitis is called diffusely spread. Such a process occupies up to 60% of the peritoneal covering. When more than 5 anatomic areas or 2 floors of the abdominal cavity are involved, which constitutes more than 60% of the peritoneal covering, peritonitis is termed generally spread. Generalized peritonitis is the total involvement of all the areas of the parietal and visceral peritoneum. Continuous spread of the infection along the peritoneum is accompanied by deterioration in the disease phase. Local unlimited and diffuse peritonitis correspond to the reactive phase which quickly moves into the toxic phase and as the process spreads and moves into the general or generalized phase, the condition reaches the terminal phase. The reactive phase of peritonitis persists for 12-24 hrs and is characterized by intensive inflammatory changes in the peritoneum. Patients complain of pains in the stomach, which are intense and are initially located at the source of peritonitis, the pain later spreads to adjacent areas and can involve half or even the whole abdomen. Vomiting of stomach contents and later of bile is a common occurrence. General clinical symptoms include a rise in body temperature up to 38 °C and above, tachycardia (pulse rate of up to 120 beats per min), increase in blood pressure and respiratory rate (up to 24-28 per min), restlessness, motor agitation. The face is initially flushed, then becomes pale. The abdomen is retracted or slightly distended; the abdominal wall or half of it is not involved in the act of breathing. On palpation the patient demonstrates severe tenderness and tensing of all the abdominal muscles depending on the spread of the process along the peritoneum. Bowels sounds are absent on auscultation. Laboratory blood tests show leucocytosis with a mild shift of the leukocyte formula to the left. The toxic phase of peritonitis persists for 24-72 hrs and is characterized by severe intoxication and paresis of the GI (tract). Patients become adynamic, gaunted and hollow-eyed, skin is pale. Pulse rate is more than 120 beats per min and weak, blood pressure reduces. Body temperature is high (39-40 °C) hectic in nature, patients sometimes have chills. Abdomen is distended, tender on palpation but muscle rigidity is less than in the reactive period, abdominal percussion reveals meteorism, bowel sounds are absent. Vomiting is common of the intestinal contents. Blood tests show leucocytosis with a marked shift of the leukocyte formula to the left (the appearance of immature forms) and toxic granular leucocytes. The phase of polyorganic failure (after 72 hrs) is characterized by extreme intoxication of the organism. The patient is depressed, adynamic, apathetic to his surroundings, may be confused, quiet often develops toxic psychosis (inadequate behavior, agitation and hallucinations). The face is grayish-yellow, livid, bluish or sunken (Hippocratic face). There is profuse vomiting with the odour of faeces. The pulse is fast, weak and thready, blood pressure is low. Abdomen is very distended, tender to palpation all over. Peristaltic bowel sounds are absent («grave silence»). The body temperature reduces; the skin is covered with cold sweat. Blood tests show leucocytosis with a marked shift of the leukocyte formula to the left. Urine output is reduced, with a high proteinuria and cylinders present. Peculiarities of the examination of the patient with peritonitis. When the infection spreads to the peritoneum from an inflamed abdominal organ the signs of peritonitis add to the signs of the originally infected organ that happened to be the cause of infection. Subsequently when the process spreads and moves into the next phase, it becomes difficult to establish the original source of infection. Patients with peritonitis complain of abdominal pains, thirst, weakness, vomiting and dyspnea. Pain is persistent and the location differs according to the source of infection at the onset of the disease, then the pain spreads to half or the entire abdomen. When fluid accumulates in the subphrenic space, the pain can radiate to the shoulders, scapula; and if it accumulates in the pelvis - there is pain in the rectum and perineum. Pain can increase gradually (when an organ is inflamed) or suddenly and become intense when a hollow viscus perforates, as in stomach and duodenal ulcers. The character and location of pain depends on the main (original) disease: for example in acute cholecystitis the pain is griping and located in the right hypochondria, in acute intestinal obstruction the pain is intense, colicky and with the onset of peritonitis (paresis of the intestines), it reduces in intensity and becomes persistent. Inspection reveals a patient with sunken hollow eyes, pale, sharpened face, with fast breathing. Pulse is rapid and increases as the disease progress, blood pressure reduces, dry and coated tongue. The abdomen is initially not changed or just a little distended. Extreme distension is found in fullblown peritonitis. It is not involved in the act of breathing or some part of it is left out, breathing becomes shallow and intercostal. In peritonitis caused by ruptured viscus, the abdomen can be retracted at the initial stage of the disease. Peristaltic bowel sounds are absent during the toxic and terminal phases. A high tympanic sound is heard on auscultation of the abdomen, it is dull over the areas of fluid accumulation. During the initial phases there is tenderness over the areas of the source of infection, this later spreads over several areas, half or the entire abdomen. One of the vital symptoms of peritonitis is abdominal guarding. To elicit this symptom both hands are used to palpate the abdomen gently, placing the palms over two symmetrical areas of the abdominal wall. Moving the hands over the abdominal wall with minimal pressure the amount of resistance from the muscles on both sides is compared: tensing of the abdominal wall and resistance from it indicate the presence of muscular rigidity. Intense muscular rigidity is encountered in perforations of viscus (board-like stomach). The cause of guarding is involuntary resistance, reflex reaction of the abdominal wall caused by pain. Together with abdominal guarding a constant feature of peritonitis is rebound tenderness, the Shotkin-Blumberg's sign. This sign is based on the increase in pain on shaking the peritoneum. To elicit this sign the abdominal wall is pressed deeply and gently using the fingers and then the pressure is quickly released. The resulting irritation of the peritoneum causes severe pain at affected area which is a sign of peritoneum inflamation. Laboratory blood tests show leucocytosis, which can reach up to 15-20x109/l with a shift of the leukocyte formula to the left, anemia; ESR is high; protein and cylinders are present in the urine. Plain abdominal x-rays can show free gas if peritonitis resulted from a perforated viscus; in ileus there are distended intestinal loops with fluid accumulation in them. To establish the diagnosis of peritonitis, several symptoms have to be present of which the most reliable are: abdominal pains, tenderness on palpation, guarding or rigidity of the abdominal wall muscle, Shotkin-Blumberg's sign, dry tongue, rapid pulse, high body temperature, deficit of pulse versus temperature, high leucocytosis with a shift to the left, the presence of free gas in the abdominal cavity. To confirm the diagnosis in unclear situations and to establish the source of infection, laparoscopy is done. After the diagnosis has been established the spread of peritonitis as well as its phase of development are determined. Treatment. Purulent peritonitis is an indication for emergency operation. The objective of surgery is to liquidate the source of infection, sanitation of the abdominal cavity and evacuation of the purulent exudate in the abdominal cavity or the contents of the GIT in case of perforated viscus, drainage of the abdominal cavity for the infusion of antibiotics and evacuation of exudate. The preoperative assessment must be short - not more than 2 hours and aimed at the restoration of blood circulation, improvement of water-electrolyte imbalance and restoration of the circulating blood volume. Evaluation of the cardiovascular system during the preoperative period is especially important in patients who frail and elderly and who as a result of the severe intoxication easily develop cardiac decompensation (ref. Chapter VII). In spreading peritonitis the best surgical approach is the mid-line laparotomy incision. Liquidation of the source of infection involves the excision of the affected organ (appendectomy, cholecystectomy, removal of fallopian tubes, resection of the intestine etc.), closure of the perforation in the case of stomach or duodenal ulcers. Sanitation (toileting) of the abdominal cavity is aimed at evacuation of the exudate with the help of electric suction machine (fig. 113) or dry cleaning the abdominal cavity with gauze swabs, clearing of the fibrin deposits, washing the abdominal cavity with antiseptic solutions (dioxidin, soluble furagin, sodium hypochloride, ultrasonic cavitation). To combat the intestinal paresis the intestines are decompressed. In intestinal resection decompression is done through the open ends of the bowel: the bowel is brought out of the abdominal cavity, the clamps are removed and by pressing down the bowel contents and gas are emptied. In case one or both ends of the bowel are brought out in the form of a fistula, decompression will be achieved after the operation through this fistula (enterostomy or colostomy). Where the source of peritonitis is liquidated without opening the lumen of the intestines (appendectomy, cholecystectomy, closure of a perforation), then decompression of the intestine during and after the operation is achieved by using soft long small-intestinal tubes with lots of holes on the sides which are passed through the nose, oesophagus, stomach and into the small intestine at the time of operation. This tube can be pushed into the small intestine during laparotomy as well; through it the intestinal contents are evacuated and left in situ for long-term decompression during the postoperative period. Decompression, which is continued into the postoperative period is aimed at evacuating the intestinal contents in order to prevent them from being absorbed into the organism and to prevent intoxication, as well as to reduce the extent of circulatory and nutritional imbalance in the intestinal walls that have been overstretched by gas. Moreover, the distended abdomen impedes the excursion of the diaphragm and causes the shift of the heart and lungs leading to cardiac and respiratory dysfunction. After deflating the intestines, 150 mls of 0.25% solution of novocain are injected into the mesentery of the small bowels.
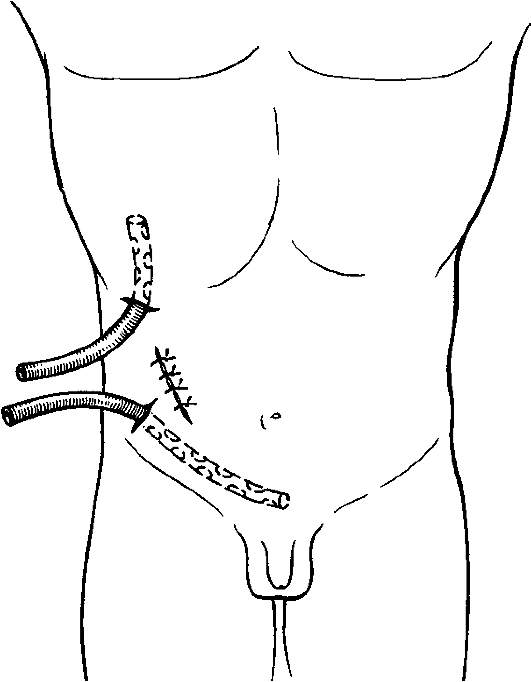
Fig. 113. Electric suction of exudate in peritonitis. The operation is completed by abdominal drainage (fig. 114). Vinyl chloride or silicone drainage tubes with a diameter of 0, 2-0, 8 cm are used. The tubes are passed through separate punctures in the abdominal wall. The laparotomy incision is normally sutured tight. In generalized peritonitis drainage tubes are inserted for periodic (fractional) irrigation of the abdominal cavity during the postoperative period with antiseptic solutions. This method of continuous-flow peritoneal dialysis is only used in situations when it was not possible to fully evacuate all the purulent exudates and also in terminal stages of peritonitis (fig. 115, 116).
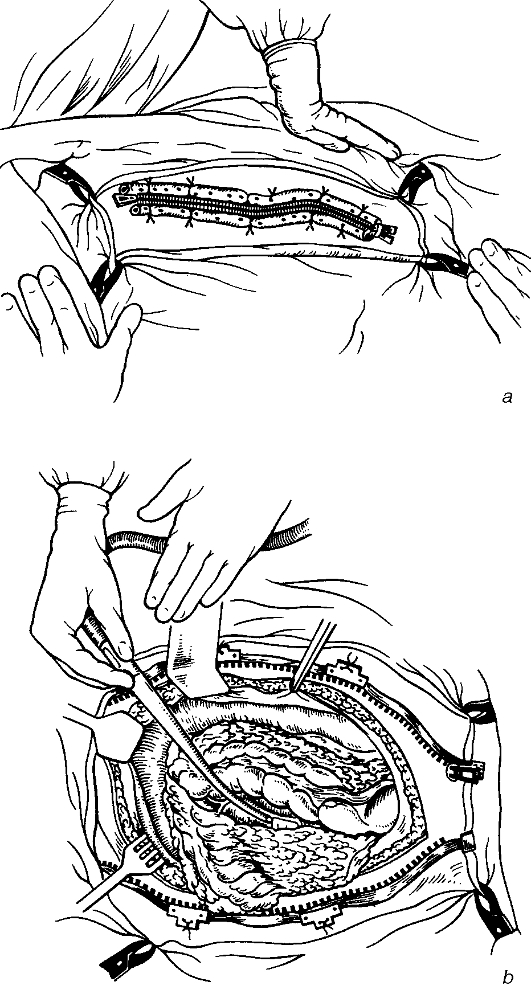
Fig. 114. Abdominal drainage in destructive appendicitis complicated by local peritonitis. Repeated toileting of the abdominal cavity in generalized peritonitis can be done by means of laparostomy. To do this, the operation is completed by suturing a zipper along the wound edges. After the operation the zipper is periodically opened, the exudate is aspirated, the abdominal cavity is washed with antiseptic solutions (fig. 117). This procedure is continued till complete eradication of inflammation in the abdominal cavity, the zipper is then removed and the wound is sutured. Treatment of patients with suppurative peritonitis in the postoperative period is focused on the following: 1) toileting (sanitation) of the abdominal cavity; 2) antibacterial therapy; 3) detoxication therapy; 4) reestablishment of metabolic balance of blood (water-electrolyte, acid - base balance, protein composition and the circulating blood volume); 5) restoration of intestinal peristalsis.
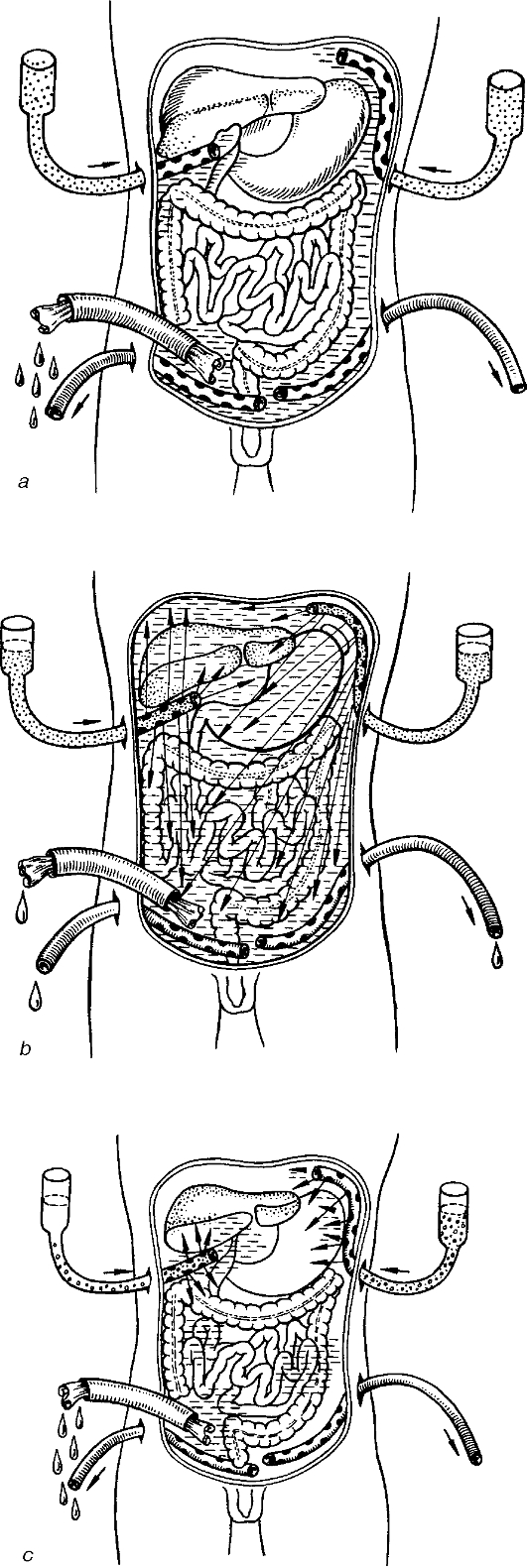
Fig. 115. Peritoneal lavage: a - appropriate technique; b and c - inappropriate lavage as a result of a decrease in dialysate outflow.
Fig. 116. The optimum patient's position during peritoneal lavage.
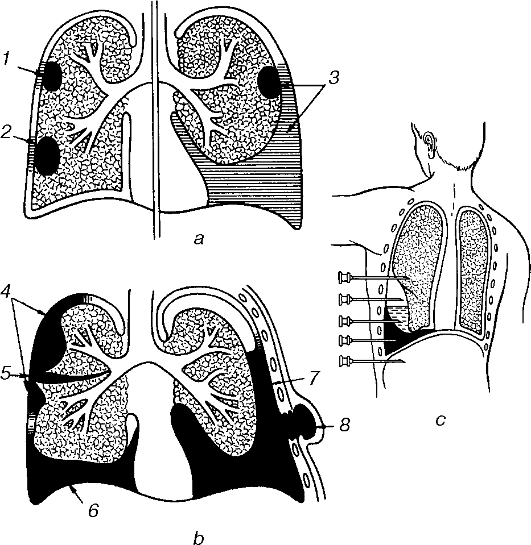
Fig. 117. Laparostoma (a) followed by elective (scheduled) cleaning the abdominal cavity (b). During the postoperative period before the intestinal functions are fully restored the patient is placed on complete parenteral feeding (ref. Chapter VI «Blood components, blood products and nutritional support»). As the intestinal functions are restored, the patient is gradually returned to enteral feeding. To ensure detoxication, blood substitutes with detoxication properties are given as well as forced diuresis, haemadsorption, plasmapheresis etc. are used. ACUTE SUPPURATIVE PLEURISY (PLEURAL EMPYEMA) Suppurative (purulent) pleurisy (pleural empyema) is the suppurative inflammation of the parietal and visceral pleura that is associated with local changes and intoxication. Classification 1. According to the etiology: streptococcal, pneumococcal, staphylococcal, diplococcal, mixed etc. 2. According to the pus distribution: free-total, average, minimal, encapsulatedsingle or multiple chambered (basal, attached to the pleural wall, paramedisternal, interlobar, and apical). 3. According to the character of the pathological changes: acute suppurative, ichorous, puruloichorous, pyopneumothorax and hemopyothorax. 4. According to the presenting clinical features: acute and chronic. Supurative pleurisy is a secondary disease (fig. 118) that often occurs as a complication of infectious processes in the lungs - croupous or postinfluenzal pneumonias. Para and metapneumonic suppurative pleurisy are identified. Parapneumonic pleurisy is a complication of pneumonia at the height of the disease process whereas metapneumonic or postpneumonic occurs after the pneumonia has resolved. Metapneumonic pleurisy is more common than parapneumonic and is mostly associated with the development of seropurulent or purulent effusions. Contamination of the pleural cavity can occur through lymphogenic or haematogenous spread from non-pulmonary sources of infections (suppurative appendicitis, suppurative cholecystitis, pancreatitis, retroperitoneal phlegmon etc.). This type of infection occurs rarely and starts with the formation of serous effusions which later change into seropurulent and purulent. The most common cause of purulent pleurisy is acute lung abscess. Contamination of the pleural cavity in such a situation is by direct contact, lymphogenic or through the rupture of the abscess into the pleural cavity with formation of pyopneumothorax. Primary suppurative pleurisy occurs from penetrating chest injuries.
Fig. 118. Purulent pleurisy: thoracic empyema (a, b); pleurocentesis, typical errors (c). 1-3 - superficial pulmonary abscesses with pleural adhesions; 4 - sacculated empyema; 5 - interlobular empyema; 6 - diaphragmatic empyema; 7 - pyopneumothorax; 8 - empyema necessitatis. Acute suppurative pleurisy is divided into primary and secondary: according to the pus distribution - free (total, average, minimal), encapsulated (single or multiple chambered, interlobar, and apical); according to the character of the exudates: purulent, ichorous, puruloichorous. The clinical presentation of the disease features: 1) symptoms of the main disease that gave rise to pleurisy; 2) signs of suppurative intoxication; 3) symptoms resulting from the accumulation of fluid into the pleural cavity. Patients with suppurative pleurisy complain of pains in the side of the chest, cough, a feeling of fullness or heaviness in the side, difficulty in breathing, being unable to inhale deeply, dyspnea, a rise in body temperature and weakness. Chest pains are more intense at the onset of the disease, are felt as piercing and as the disease progresses and more fluid is accumulated, pain reduces and there is a feeling of heaviness in the side. Dyspnea gradually worsens. Cough as a rule is dry, but when the process is secondary to lung abscess or pneumonia, mucous or purulent sputum is coughed out, sometimes in large quantities. When pleurisy sets in, the character of cough changes from that in the original disease; cough becomes more persistent, violent, disturbing the patient mostly in the night, it may become paroxysmal and tends to increase on lying on the affected side. Dyspnea can be extreme, increasing like the pain when the patient sleeps on the healthy side. Therefore, the patients are forced to sleep on the sick side, which makes breathing easier and reduces the chest pains. Body temperature rises to a high level (39-40 °C), and is of constant or hectic character. Pulse rate reaches 120-130 beats/min, which indicates both suppurative intoxication and a shift of the heart and mediasternum vessels to the healthy side as a result of the fluid accumulation. The rupture of a lung abscess situated beneath the pleura with the entry of pus and air into the pleural cavity is associated with the development of pleural shock. The rupture is preceded by a strong persistent cough that ends with the appearance of intense sharp pain in the side of chest. The patient cannot breath in deeply; the face becomes pale and is covered by cold sweat. Pulse is rapid and weak, blood pressure decreases. Breathing is shallow and fast because of the extreme pain, there is acrocyanosis and dyspnea worsens. The reason for this serious clinical picture is the pleural irritation, which causes pain, the pressure on the lungs exerted by pus and air, the shift of organs in the mediasternum to the healthy side with its accompanying disturbance of cardiac functions. After the acute phase has subsided and the patient has been helped to overcome shock, intoxication develops; this intoxication is more severe than those which occur during parapneumonic and metapneumonic empyema of the pleura. As this condition being secondary to an inflammatory process elsewhere in the body so, at the time of anamnesis investigation one should take note of functional disorders that occurred during the original disease: chest pains located at the sides, change in the character of cough, difficulty in inhalation, a rise in body temperature, increasing weakness, malaise or the appearance of a sudden sharp pain in the side of chest. General examination of the patient reveals pallor, dyspnea, and uncomfortable position in bed - half-sitting or on the side. Sometimes the patient is found to be pressing on the side, which reduces the pain on inhalation. Breathing rate increases to 20-25 and in extreme cases to 30-40 per min. Inspection of the chest reveals limitations in the breathing excursion of the chest with the sick side impaired or even not taking part in the process. When large amounts of fluid are accumulated in the pleural cavity, a swelling in the posterior lower parts of the chest is found and the intercostal spaces are filled up. Palpation of the intercostal spaces causes some tenderness. Tactile fremitus on the affected side is reduced or is not determined at all. Percussion of the chest reveals dullness in the percussion note over the areas of accumulation, in total pleural empyema there is dullness over the whole half of the chest, in case of large amounts of accumulation (but not total), the upper level of dullness is located on the C-shaped Ellis-Damoiseau's line. In this situation the Garland's triangle and Grocco's-Rauchfuss' triangles are determined. Percussion also reveals the shift of the mid dullness towards the healthy side, which indicates the shift of the mediasternum exerted by the accumulated fluid in the pleural cavity. Auscultation reveals a marked decrease in breath sounds or their total absence over the areas of accumulation. Blood tests show leucocytosis, a shift of the leukocyte formula to the left and a high ESR. Body temperature increases to 38-40 °C, and is of a constant or remittent hectic nature. X-ray examination (roentgenoscopy and roent-genography) is done to determine the presence of fluid in the pleural cavity. The x-ray shows the amount and location of the fluid. At the beginning of the disease fluid accumulation is at the posterior lower parts of the pleural cavity - in the costodiaphragmal sinus, as the fluid increases, the shadow over the lung field increases as well. In hydrothorax, the fluid accumulation in a pleural effusion has a C-shaped border and never assumes a horizontal level. In pyopneumothorax a free layer of gas is evident over the horizontal level of fluid in the pleural cavity. These physical and x-ray investigations help to establish the correct diagnosis of pleural effusion. The increased body temperature as well as severe intoxication; changes in the blood picture (leucocytosis and a high ESR) are all signs of the development of suppurative pleurisy. To confirm the diagnosis of suppurative pleurisy, determine the causative agent and carry out the proper antibacterial therapy a diagnostic puncture of the pleural cavity is performed. The point for puncture is chosen at the area of maximum tenderness, a typical point is in the eighth or ninth intercostal space in-between the scapular and posterior axillary lines. In limited and encapsulated pleurisy, small amounts of fluid accumulations, the puncture point is determined together with the radiologist during the roentgenoscopy investigation. A 20 ml syringe and 0, 5, 1 and 2 mm diameter needle, a three-way cock, a 0, 5% solution of Novocain are needed for the puncture. The procedure is similar to that for surgery: the hands are scrubbed, and sterile gloves are used. The patient is put in the sitting position on a table with the trunk slightly bent and the back out. The nurse or assistant stands in front of the patient and holds him in position. The back is cleaned with antiseptics; using a small needle the skin and the deep lying tissues are anesthetized. The needle is then changed for a bigger one (1-2 mm), the skin is pierced, displaced slightly to the side, and the needle is pushed along the upper side of the lower rib sending forth a jet of Novocain. A sure sign of the needle being inside the pleural cavity is the fact that it no longer encounters any resistance as it did when piercing the parietal pleura. The aspiration of a purulent fluid confirms the diagnosis of pleural empyema. Some pus is collected into the syringe, the three-way cock is closed at the needle and the syringe disconnected, the contents are put into a tube and sent for laboratory and bacteriological investigations, evacuation of the fluid is then continued until a negative pressure appears in the syringe. Treatment. Treatment of suppurative pleurisy involves the evacuation of pus, fighting the infection, detoxication therapy and the restoration of impaired organ functions. The prompt eradication of foci of suppurative pleural infection and the expansion of collapsed lungs helps to achieve the main aim of treatment - restoration of the close contact between the visceral and parietal pleura and their union. The subsequent obliteration of the suppurative cavity leads to healing of the patient. The earlier treatment is started for a pleural empyema the better the outcome, since in that way irreversible changes do not have time to develop in the collapsed lung, nor does thick fibrous deposition (pleural plagues) have a chance to form in the inflamed pleura. In the presence of this thick fibrous layer (plagues) the lung cannot fully expand and some amount of space with thick walls is left over in between the pleura, which results in the acute process turning into a chronic one. The main method used to treat a pleural empyema is the closed method, during which the pleural cavity is not opened. In the open method the chest is opened through a wide incision for the evacuation of pus and fibrin deposits and plagues (decortication). The closed method of treatment of pleural empyema includes therapeutic puncture and drainage of the pleural cavity by way of pleural taps through the chest drainage tube. The drainage tube can also be passed through the bed of a resected rib, suturing the surrounding soft tissues around the tube to create an airtight condition (fig. 119, 120).
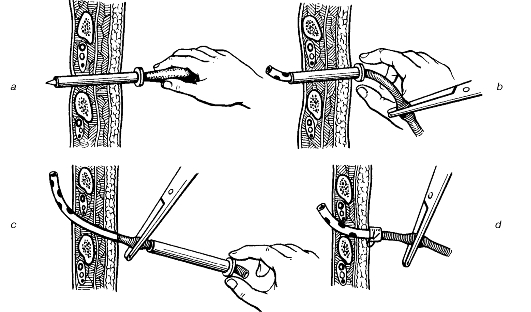
Fig. 119. Pleural drainage using a trocar: a - pleurocentesis; b - insertion of the drain through the trocar's cannula; c - removal of the trocar's cannula; d - fixation of the drain. Treatment of suppurative pleurisy is started with a pleural tap. It is a must to do it under local anesthesia. A wide bore needle (1 - 1, 5 mm) has to be used; a three-way cock is necessary as well as a rubber tube with a clamp to close the needle when the syringe is disconnected. This helps to prevent pyopneumothorax, which can result from the entry of atmospheric air into the pleural cavity. The evacuation of pus, especially in the case of massive effusion should be done gradually, so as not to cause the development of hyperemia ex vacuo and a sharp shift of the mediasternum. This can lead to the development of shock. Evacuation of the fluid is continued until a negative pressure appears in the syringe (when drawing back the piston, fluid does not appear and when the syringe piston is released, it returns to its original position). Pleural drainage is completed by the infusion into the cavity of proteolytic enzymes and antibiotics. Puncture is repeated daily. When the first puncture is not successful, active constant aspiration of pus from the pleural cavity can be employed. Permanent drainage tubes are placed into the pleural cavity. To achieve this the skin is first anesthetized, scalpel is used to make a stab incision in the skin, a wide trocar is pushed into the pleural cavity through the intercostal space, the stylet is removed and the drainage tube is passed through the trocar into the cavity, whereupon the trocar is also removed. The drainage tube is fixed to the skin either by sutures or adhesive plaster and the tube connected to a closed drainage system at a constant vacuum of 50-100 mm of H2O, using the flowing water system or an electric aspirator. Pus from the pleural cavity is evacuated constantly and with the help of the negative pressure the two pleural layers unite and stick together, thereby eliminating the suppurative cavity (fig. 121).
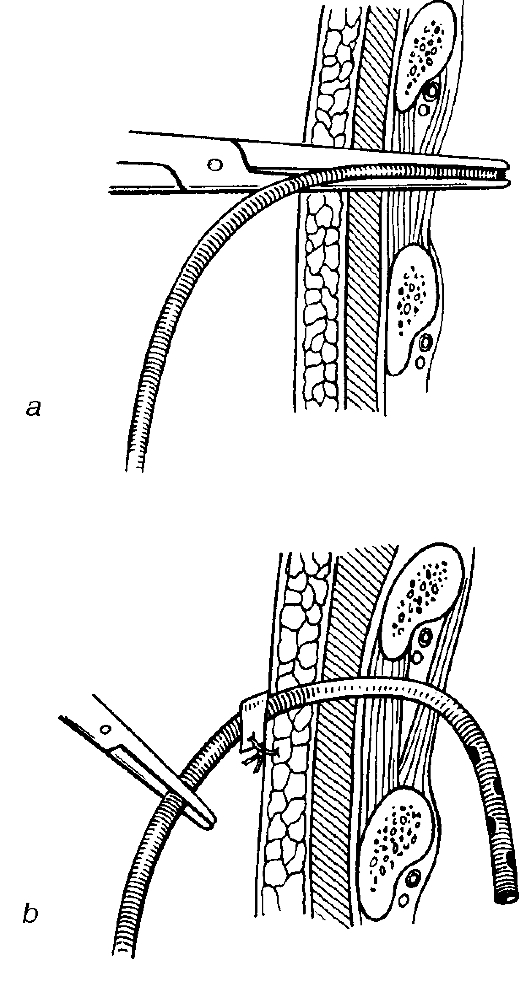
Fig. 120. A type of closed pleural drainage in purulent pleurisy: a - insertion of the drain using haemostatic forceps; b - fixation of the drain.
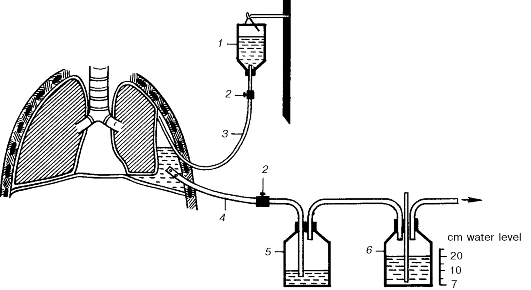
Fig. 121. Vacuum pleural drainage in purulent pleurisy: 1 - drainage solution; 2 - rack; 3 - through drain; 4 - suction drain; 5 - vessel for exudate; 6 - water vacuummeter; 7 - the site for connection with VK1 compressor.
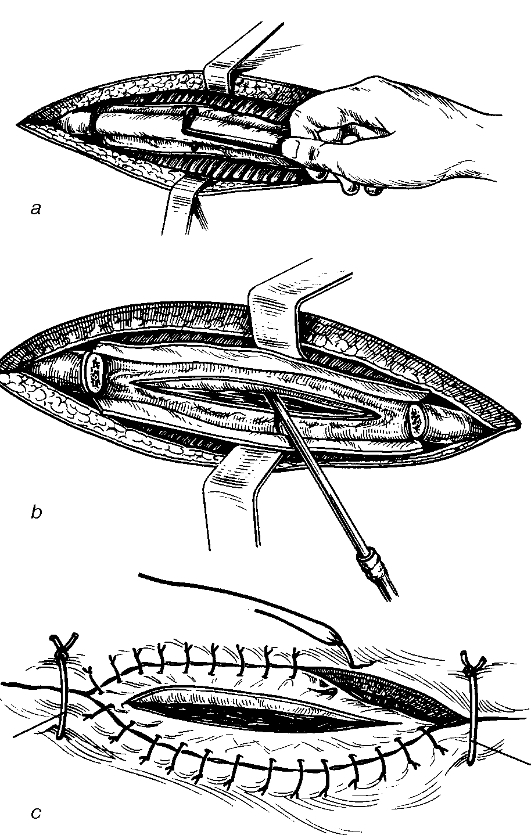
Fig. 122. Thoracostomy: a - subperiosteal resection of the rib; b - dissection of the resected rib's bed followed by opening the pleural cavity and suction of pus; c - making the thoracostomy followed by suturing the periosteum with cutaneous wound margins. The costal ends are covered with the periosteum and soft tissues sewn with removable sutures through all the layers of the wound (1, 2). When it is not possible to provide for a constant drainage, a valve made of glove rubber is slipped over the tip of the drainage tube, which is then placed into a bottle with antiseptic (Buelau's method of siphon drainage). The valve allows pus and air (in case of pyopneumothorax) to flow into the bottle, and closes when there is a negative pressure in the pleural cavity, preventing air and fluid back into the pleural cavity during inhalation. In rare cases when the closed method is ineffective, the open method is applied - thoracotomy for the evacuation of the thick pus, fibrin, sequestra of lung tissue which cannot be removed through the needle or drainage tube (fig. 122). |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 91; Нарушение авторского права страницы