|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Acute suppurative diseases of soft tissues (soft tissue infections)
Abscess (boil). This is a localized accumulation of pus in different tissues or organs resulting from suppurative tissue disintegration and cavity formation unlike an empyema, which involves the accumulation of pus into natural body cavities and cavities of hollow organs. The agents of infection are normally staphylococci in the form of a monoculture or in association with other microbes - E. Coli, proteus, streptococcus, bacterioides etc. The infectious agents normally enter the organism from outside (exogenic infections), but can also invade the body from within (endogenic) - as for instance, when the organisms enter from neighboring or distant organs, metastatic abscesses in cases of sepsis. Abscesses can result from the injection into tissues of concentrated solutions of drugs - 25% solutions of magnesium sulphate, 24% solutions of cordiamin, 50% solutions of analgin etc. The development of suppurative inflammation leads to tissue disintegration and sometimes necrosis with rejection of the dead tissues - sequestration. Sequestra can subsequently dissolve when acted upon by enzymes. The form of the abscess cavity can be a simple one or complex with several pockets. The abscess wall is initially covered with purulent fibrinous deposits and fragments of necrotic tissues. Then an inflammation zone develops at the periphery leading to the formation of the pyogenic membrane made up of connective tissue. An abscess that has resulted from a suppurative or aseptic inflammation can have different outcomes: spontaneous opening (burst) outside (abscess of the subcutaneous fatty layer, abscess of the muscles, mastitis, paraproctitis etc.), burst opening of an abscess into a closed cavity (abdominal, pleura, in a joint space etc.). An abscess can also open into a hollow cavity that has a connection to the outside (the intestinal lumen, the urinary bladder etc.). Under favourable conditions an abscess cavity decreases in size after the pus has evacuated, collapses and heals up by scarring; when evacuation is not complete the process can develop into a chronic one with formation of a fistula at the site where it burst. Superficially located abscesses are marked by redness, swelling, pain, local rise in temperature, functional disorders and sometimes fluctuations can be elicited. The sites of infection may vary in size. The characteristics of the pus contained in an abscess cavity (consistency, colour and odour) depend on the type of causative agent involved: foul-smelling odour, dirty grey colour of pus is characteristic of ichorous strains; thick yellowish green pus - for staphylococcus; a bluish-green colour and sweetish smell -pseudomonas bacilli etc. General clinical features of an abscess are: a rise in body temperature from subfebrile to high, general malaise, weakness, loss of appetite and headache. The peripheral blood picture shows leucocytosis with neutrophilia and a shift of the leukocyte count to the left. ESR is raised. Signs of intoxication that occur in cases of serious abscesses can result from the absorption of toxic products from the focus of infection (suppurative resorptive fever), as well as from the development of sepsis (see «Sepsis»). An abscess has to be differentiated from haematoma, cysts and tumor degenerations. Diagnostic puncture can play a very important role here: when pus is obtained in this procedure it not only helps to establish the diagnosis in unclear cases but also can be sent for bacteriologic analysis - to isolate the agent and to determine its sensitivity to antibiotics. The presence of gas - producing bacterial strains lead to the accumulation of gas in the abscess cavity, so-called gaseous abscess. Percussion over such an abscess gives a tympanic sound; X-ray films show the presence of gas bubbles with horizontal fluid levels beneath them (it is often observed in abscesses caused by agents of ichorous infections). Treatment of an abscess is by incision, evacuation and drainage of the abscess cavity. Cold tuberculous abscesses are not to be incised since there is always the danger of causing superinfections by suppurative strains. Small abscesses with well-formed capsules have to be removed in whole without first opening them. An abscess has to be incised using the shortest surgical approach based on the anatomic and topographic peculiarities of the organ. Not infrequently an abscess is opened along a needle: the abscess is initially punctured with a needle, then the incision is made along the needle into the abscess cavity. The incision has to be made as much as possible towards the lower poles in order to create better conditions for drainage. In order to reduce contamination of the surrounding tissues during the process of incision, the surgical field is well isolated by gauze or napkins and after a small incision into the cavity an electric suction machine is used to evacuate the pus. After the pus has been suctioned, the incision is increased, the cavity is explored by using the finger, breaking in the process the lacunae, and tissue sequestra are removed. All manipulations should be done carefully, so as not to destroy the pyogenic membrane. The abscess cavity is washed with an antiseptic solution, and then drained with one or several plastic or PVC tubes, or gauze swabs soaked with some proteolytic enzymes and antiseptics are packed into the cavity for drainage purposes. If drainage through the main incision is not adequate, another one is made on the opposite side - counter-aperture. Treatment of abscesses after incision and drainage is identical to that for treating infected wounds. General therapeutic measures include body fortifying therapies, blood and plasma transfusions, and prescription of antibiotics taking into consideration the sensitivity results of the microbiologic analysis, specific therapeutic modalities (immunization with staphylococcal anatoxin, specific anatoxin etc.). Phlegmon. This is an acute diffuse suppurative inflammation of the subcutaneous fatty tissue without localization. Depending on the locality, phlegmon is divided into subcutaneous, intra muscular and retroperitoneal. Phlegmons of certain locations have specific names: suppurative (purulent) mediastinitis, paraproctitis, paranephritis, paraarticular phlegmon etc. Phlegmon that develops from the spread of a suppurative infection from the lymph nodes is known as an adenophlegmon. Phlegmons tend to spread through the subcutaneous space, vascular beds and along the fascia lodge. Phlegmon starts with the development of serous infiltration of the fatty layer. The exudate quickly assumes a suppurative nature, areas of necrosis are formed, which later join together. Necrosis and the fatty dissolution lead to the formation of a phlegmonic abscess. Signs of phlegmon are similar to the general symptoms of suppurative-inflammatory processes (a rise in the body temperature, weakness, malaise, and headache). These determine the patient's complaints, there is also pain and swelling at the site of infection, tenderness in movement as well as when changing position of the body. Subcutaneous phlegmon locally presents with the classical signs of inflammation (fig. 84, colour inset). Swelling normally increases at the beginning, the overlying skin is red and shiny and then gradually gets pale and later turns to normal. A painful induration is palpated without clear boundaries, immobile and hot to touch. When an abscess forms, the infiltrate becomes soft and fluctuation sign can be positive. Regional lymph nodes are enlarged and painful. In certain instances red stripes or bands (net or tubular lymphadenitis) can be found around the infiltration. Active and passive limb movements, turning of the head, and a change in bodily posture cause extreme pain in the area of phlegmon. In deep-seated (intermuscular) phlegmon of the limb, the limb size increases compared to the other healthy limb. A measuring tape can be used to gauge the exact increase in limb size. Sometimes the tissues in the area of the phlegmon get enlarged. A deep extremely painful infiltrate is palpated. An attempt to move the limb may cause severe pain, a defensive (tender) muscle contracture can be encountered in the form of a forced positioning of the limb in a less painful position. Regional lymph nodes are enlarged and painful. When pus is aspirated during puncture it confirms the diagnosis of intermuscular phlegmon. In the neck region suppurative inflammation with mild general clinical symptoms of infection can appear in the form of a wood-hard infiltration - woody phlegmon. The infiltration is not very painful, fixed to the skin, fascia and aponeurosis and absolutely immobile, increase in size is very slow. Suppuration of the infiltrate occurs rarely. The disease process is very slow, with subfebrile temperature and a very mild form of intoxication. Treatment of phlegmon is surgical. It is only at the initial stage when the process is still assumed to be a serous inflammation that conservative therapy can be allowed: this includes bed rest, rest of the affected limb, antibiotic therapy, ultraviolet irradiation therapy as well as electrophoresis with chemotrypsin. Novocain block of fascial case with antibiotics by the Vishnevsky method is usually effective. The improvement of the patient's general condition, diminishing local signs of inflammation are indicative of the process being localized or regressing. In the absence of positive effect within 12-24 hours or in the case of deterioration of symptoms the patient must be operated upon. Patients admitted to hospital in the advanced stage of the disease, those with severe intoxications, progressive symptoms and those with purulent infections are operated upon as emergency. The phlegmon is incised under general anesthesia; pus and necrotic tissues are evacuated. Purulent tracts and pockets are opened; the wound is thoroughly washed with antiseptic solutions and drained. To ensure adequate drainage extra incisions (contra-apertures) are sometimes made. Treatment after surgery is similar to that for treating infected wounds. Furuncle (pimple). This is an acute suppurative-necrotic inflammation of the hair follicle of the sebaceous gland and the surrounding subcutaneous fatty layer. Furuncles are mostly found at the back of the neck, forearm, the dorsal aspect of the hand and fingers, the face and the thigh. The appearance of two or more furuncles suggests furunculosis. In the development of a furuncle, micro trauma e.g. scratching of the skin during diseases that are accompanied by itching plays an important role. The hair bed initially gets inflamed, as does the sebaceous gland, which later on together with surrounding tissues get necrotic to form a necrotic core around which the inflammation infiltrate is centered. In the early stage of the inflammatory process patients complain of the development of a painful pustule or tender induration in the thick of skin. With a progression of the disease general malaise sets in, the body temperature rises and the pain in the area of growing induration also increases. Furuncles that occur in areas such as the scalp, occipitus, external ears and the dorsal aspects of the fingers, where the skin is closely fixed to the underlying tissues, are the most painful. Examination at the onset of the disease reveals a small pustule with surrounding skin hyperemia. Rarely an induration deep in the skin is found with the overlying skin hyperemic, pus at this stage is absent. As the process continues, there appears above the surrounding skin a cone - shaped infiltrate 0, 5-1, 5 cm in diameter, which has no clear boundaries. The overlying skin is of purple - red colour. In the center of infiltration there appears a soft area covered by a scab, with small amounts of pus oozing out beneath the scab. After evacuation of the pus some greenish coloured area of tissue is noticeable - apex of the necrotic core. With the development of the necrotic core the quantity of pus increases, and the core is evacuated with the pus and blood. After the core has been cleared, a fairly deep wound with a mild bleeding tendency is found in the center; this is quickly filled with granulation and heals over after 2-3 days with the formation of a depressed scar. Sometimes a round, soft swelling with minimum pus is found during examination at the site of the furuncle. This is a furuncle with an abscess formation as a result of complete dissolution of the necrotic core without a point of escape for the pus. When red stripes are found to be going out from the furuncle, it suggests the presence of lymphangitis, while the enlargement and tenderness of lymph nodes on palpation points to development of lymphadenitis. Patients with furuncles on the face (upper lips, eyelids, forehead) sometimes complain of severe headaches, and high temperature (fig. 85, color inset), which are signs of the furuncle being complicated by suppurative thrombophlebitis of the facial veins. The latter is associated with purulent meningitis as a result of the infection spreading to the veins of the cavernous sinus. When such symptoms as remittent fever, intense chills, profuse sweating, delirium, confusion and skin pallor are encountered, it means the patient has developed sepsis, and the appearance of suppuration in other organs (metastatic abscess) confirms the diagnosis of septicemia (septicopyemia). Furuncles are treated conservatively. Patients are to be informed of the possibility of developing serious complications should they attempt to pick the lesions or cut them with a blade or even apply a hot compress. In the early stage of the process a 70% solution of alcohol is used to clean the skin, 2% alcohol solution of salicylate, and ultraviolet radiation therapy is applied. After they have opened up, dressings are put on with proteolytic enzymes, hypertonic solutions of sodium chloride and ultraviolet irradiation is applied. When the core is evacuated, dressings with synthomycin ointments, or methyluracyl are applied. When the furuncle is associated with such complications as lymphangitis and lymphadenitis, antibiotic therapy is indicated. Patients with furuncles of the upper lip and above it have to be hospitalized as emergency in the surgical unit for general and topical therapy including antibiotic therapy. The condition is treated by bed rest and a diet of mashed foods. If the furuncle turns into an abscess it has to be removed through incision and drainage. The patient with recurrent furuncle at the same place has to be examined specially to rule out any metabolic disorders (diabetes mellitus, vitamin deficiency). To boost the body's resistance to staphylococcal infections, immunization is done with staphylococcal anatoxin. Carbuncle. This is an acute diffuse suppurative-necrotic inflammation of several hair follicles and sebaceous glands accompanied by the development of a common infiltration and necrosis of the skin and the surrounding subcutaneous fatty tissue as a result of vascular thrombosis. Patients complain of severe pain, the presence of a tender infiltration, a rise in body temperature, chills, malaise, weakness, fatigue, loss of appetite and headaches. There is normally a history of diabetes mellitus, vitamin deficiencies and malnutrition (fig. 86). Apart from the general symptoms of suppurative inflammations (rise in body temperature, rapid pulse, etc.), examination of the patients reveals the presence of violet - blue swelling at the back of the neck, back, the lumbar region, the face and rarely the extremities. Several infiltrations can be found at the onset of the disease, which later on join together to form a marked swelling rising above the skin level. The skin over the infiltration is tense and shiny with the violet-blue colouration more intensive in the center, which gradually becomes pale at the periphery. Several suppurative-necrotic pustules appear on the surface of the infiltration, which join together in the center to form an extensive area of skin necrosis (see fig. 86). The thin areas of necrotic skin open up at several places to form an opening through which the pus escapes. The infiltration is firm in consistency, very tender with pronounced edema around. Regional lymph nodes are enlarged and painful (lymphadenitis), lymphangitis is rare. If the infiltration bursts on its own with the release of necrotic tissues, a big hole is left in the center covered with grayish-green necrotic tissue with profuse pus. If during monitoring of a patient it is found that the edema is increasing, necrosis is rapidly progressing and the symptoms of general intoxication (tachycardia, headache, weakness) are getting worse, as evidenced by extreme chills, profuse sweating, lymphangitis, lymphadenitis, and thrombophlebitis, then this should be considered as an adverse progression of carbuncle with the development of phlegmon and sepsis.
Fig. 86. Facial carbuncle. Carbuncle of the face should be taken seriously, because of the possibility of infection spreading through the facial veins, through the superior orbital veins into the brain sinuses and the development of suppurative thrombophlebitis as well as purulent meningitis. Carbuncle has to be differentiated from Siberian ulcer carbuncle, which is characterized by the presence of hemorrhagic blisters, the absence of purulent discharge, a painless infiltration, extreme tissue edema; the necrotic tissue that results is black in colour and surrounded by tiny blisters with hemorrhagic contents. The blisters are found to contain the Siberian ulcer bacilli. Treatment of a carbuncle at the initial stages is conservative. It involves rest for the affected organ. If it is on the face the patient should be put on bed rest. Patients are not allowed to talk, and are given liquid food. After treating the carbuncle with 70% ethyl spirit, aseptic dressing is applied, and ultraviolet radiation therapy is prescribed. Antibiotics are administered parenterally and long-acting sulphanilamides - orally. Ineffective conservative therapy for 2-3 days with spreading necrosis, suppurative intoxication are indications for surgical treatment, which is done under general anesthesia. A crosswise incision is made over the infiltration up to the fascia and the necrotic tissues are excised throughout, separating them from the fascia and skin, the whole area being cleaned of necrosis and pus (fig. 87). The postoperative period is managed according to the principles of treating infected wounds; proteolytic enzymes can be applied for complete cleansing of the necrotic tissues. Hydradenitis is a suppurative inflammation of the apocrine sweat glands. Examination of the patient reveals a painful swelling often in the axilla, and rarely in the inguinal and perianal regions - the areas where the apocrine sweat glands are located. The personal history reveals the presence of some predisposing factors: increased sweating, poor hygiene, the use of depilator and the shaving of the axillary region. The disease is marked by sudden onset with the appearance of a small painful nodule, which increases in size up to 1-2 cm in diameter and sharply protrudes above the surrounding skin level (fig. 88, colour inset). Examination reveals a violet-red swelling. When several sweat glands are involved, they coalesce to form a firm infiltration, which can occupy the whole axillary fossa. Single nodules are superficial and fixed to the skin. After 10-15 days the center of the swelling softens up, fluctuation is noticeable, and some thick milky pus starts to discharge from the burst area. Once the pus is evacuated, healing starts with the formation of a scar. The disease tends to recur.
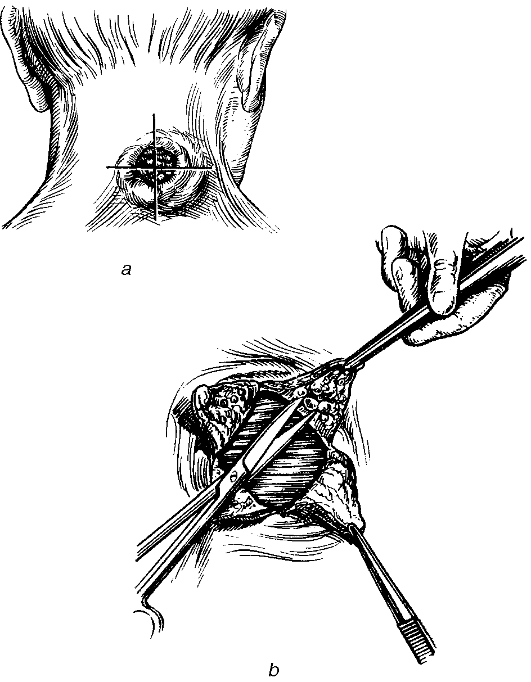
Fig. 87. Dissection of carbuncle (a) and debridement (b). When the surrounding subcutaneous fatty layer gets involved in the process, a phlegmon develops, and when the lymph nodes are involved - lymphadenitis. Unlike furuncle, the infiltration is devoid of follicular pustules or necrotic centers. Axillary hydradenitis is characterized by deep-seated infiltrations, enlarged lymph nodes, and the skin over the lesion is not firmly attached to it. Hydradenitis is treated with antibiotics, and long-acting sulphanylamides. Immunization with staphylococcal anatoxin is prescribed. The hair in the axilla is shaved, the skin is cleaned with spirit, and smeared with a 3% solution of brilliant green. Ultrasound and ultraviolet irradiation are used as physical therapeutic measures. In the case of an abscess formation, surgery has to be performed - incision and drainage. If long-term treatment of hydradenitis proves unsuccessful and there is fear of ensuing sepsis, the whole subcutaneous fatty layer of the axillary fossa is excised such as with a carbuncle. Erysipelas is a progressive acute inflammation of skin or, rarely, of mucous membranes caused by diverse Streptococcus spp. Erythaematous erysipelas results from serous inflammation at the site of invasion of the bacteria, which, in turn, leads to epidermal desquamation and detachment by inflammatory exudate with subsequent formation of blisters, or bullous erysipelas. Further, pustulous infiltration of the skin results in phlegmonous erysipelas. In addition, vascular thrombosis may cause cutaneous necrosis, or necroticerysipelas. The condition is characterised by acute onset (rigors, severe headache, tachycardia, tachypnoea, fever as high as 40-41 °C and typical signs of intoxication, i.e. insomnia, oliguria, proteinuria, haematuria, leukocyturia and hyaline and granular casts present in the urine). Marked hyperaemia (flame-like) is the major local sign of erythaematous erysipelas, which is usually accompanied by burning sensation and fever. The signs of bullous erysipelas are all those of erythaematous erysipelas accompanied by serous, purulent or haemorrhagic blisters of various size. In phlegmonous erysipelas, the local signs, i.e. hyperaemia, pain, itching, are moderate, while general ones (rigors, fever, tachycardia) may be pronounced. Necrotic erysipelas presents as black solid painless lesions of the skin at the sites of former hyperaemia, blisters or oedema. For treatment, the patient must be hospitalised. Antibacterial therapy with penicillins coupled with ultraviolet is applied as long as hyperaemia begins to subside and body temperature becomes normal. It should be noted that wet bandages, compresses or baths are absolutely contra-indicated. After cleansing with ethanol, blisters should be opened and covered by dressing with synthomycin emulsion, streptocid suspension or tetracycline ointment. Phlegmonous and necrotic erysipelas both require opening of purulent blisters, their drainage and removal of necrosis. Autodermoplasty is used to close granulating wounds. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 135; Нарушение авторского права страницы