|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
INFLAMMATION OF THE LYMPHATIC VESSELS AND LYMPH NODES
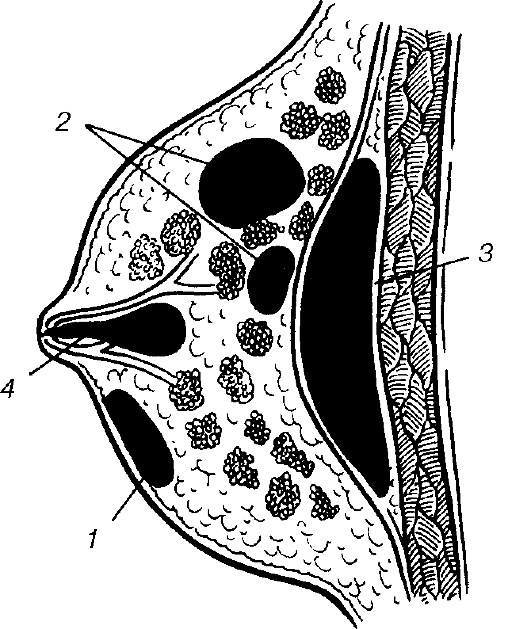
Lymphangitis is an inflammation of the lymphatic vessels that accompanies different inflammatory diseases: infected wounds and abrasions, furuncles, carbuncles, abscesses, phlegmons, panaritia etc. Lymphangitis occurs most commomly on the limbs. The appearance of lymphangitis in the course of any suppurative inflammation is an indication of progression of the main disease and a factor contributing to its aggravation. As a rule the body temperature rises to 39-40 °C, with chills, headache, increased sweating, weakness and high leucocytosis. In reticular lymphangitis, there is extreme skin hyperemia, similar to that of erysipelas but without distinct boundaries; sometime a web-like pattern is observed in the zone of marked hyperemia (fig. 88, colour inset). In trunk lymphangitis, hyperemia has the appearanace of separate bands leading from the inflamed site towards the regional lymph nodes - towards the axillary fossa or the inguinal region, the skin is edematous. Palpation reveals stripes of tender indurations in the form of strings or streaks along the lymph vessels. Regional lymph nodes are enlarged, firm, and tender to palpation. When the process affects deep lymph vessels, skin hyperemia is absent, there is pain in the limb, edema, tenderness on deep palpation and the early appearance of lymphadenitis. In the case of perilymphangitis areas of induration are found along the lymphatic vessels. Treatment is aimed primarily at eliminating the primary focus of infection and includes incision and drainage of abscess, phlegmon, pyodermia, and the rational drainage of purulent lesions. Antibiotic therapy is prescribed according to the type of microbes and their resistance to drug therapy. Rest is important, and the limb has to be elevated; for this purpose it can be immobilized. Prophylaxis of lymphangitis involves a timely and thorough primary surgical wound debridement, immobilization of the limb, and proper incision and drainage of suppurative foci as well as the rational use of antibiotics. Lymphadenitis is an inflammation of the lymph nodes resulting from a complication of different inflammatory diseases (infected wounds, furuncles, carbuncles, panaritium, erysipelas infection, osteomyelitis, thrombophlebitis, trophic ulcers etc.) and from specific infections such as tuberculosis, plague and actinomycosis (fig. 89, colour inset). The inflammation starts with a serous edema (simple, catarrhal lymphadenitis), which may evolve into suppurative and when the surrounding tissues are involved adenophlegmon develops. Acute lymphadenitis starts with the development of a tender enlarged lymph node, headaches, weakness, general ill feeling (malaise) and a rise in body temperature. The disease is not infrequently associated with lymphangitis. In catarrhal (serous) lymphadenitis the patients' general condition is only slightly affected. They complain of pains in the area of the regional lymph nodes, which are enlarged in size, firm and tender on palpation and not firmly attached to the surrounding tissues; the skin over a node is unaffected. In suppurative lymphadenitis pain is severe. Skin over the nodes is hyperemic, and the nodes are very tender on palpation. Lymph nodes, which could previously be palpated, clearly fuse together and with the surrounding tissues and become immobile. In the case of adenophlegmon there is a widespread skin hyperemia, firm infiltration without distinct borders with patches of soft areas. The body temperature rises to a high level, accompanied by chills, tachycardia, headache and pronounced weakness. In ichorous phlegmon crepitations are detected during palpation of the lesion. Suppurative lymphadenitis can lead to a spread of the infection to the subcutaneous spaces (retroperitoneal, mediasternum etc.) and sepsis. Treatment of the initial stages of lymphadenitis is conservative. It involves resting the affected organ, ultraviolet irradiation, active treatment of the primary focus of infection (timely incision and drainage of abscesses, phlegmon, proper drainage of purulent processes), and antibiotic therapy. Suppurative lymphadenitis is treated by surgery which includes incision of abscess, adenophlegmon, evacuation of pus and drainage. Postoperative therapy follows the methods of treatment for infected wounds. ACUTE MASTITIS Mastitis is an inflammation of the parenchyma and interstitial tissues of the breast. Classification of mastitis. 1. Edematous form. 2. Infiltrative form. 3. Suppurative-destructive forms: a) breast abscess; b) phlegmonous mastitis; c) gangrenous mastitis. Acute mastitis is generally encountered in breastfeeding women, during the first two weeks after childbirth (lactating mastitis). Primiparas (those delivering for the first time) suffer more than women who have had several deliveries and this is due to the narrow breast ducts, slightly mobile nipples, the friable nipple skin that is easily exposed to minute injuries. Acute mastitis is divided according to the period of the inflammatory process into serous (initial), acute infiltrative and destructive: abscess, phlegmonous and gangrenous mastitis. Early diagnosis of initial forms of mastitis and the earlier initiated treatment lead to a complete resolution of the process and prevent it from going to the purulent and destructive stage. Acute inflammatory processes in the breast are to be differentiated from acute milk stasis (congestion). Milk congestion occurs twice as often in primiparas. Patients complain of breast engorgement, heaviness and tension in the breasts, which gradually increase in intensity. Presenting masses conform to the contours of the breast lobules, and are quiet mobile, with distinct borders, the surface is not smooth and not painful. When they are pressed milk flows out easily and milking is not painful. After the milk is released the patient immediately feels relieved. The general condition is relatively not affected, the body temperature, blood test results are all within the normal values. Acute breast congestion is often bilateral and occurs at the time of profuse milk secretion (on the 2nd-5th day after delivery). It is not always easy to differentiate congestion from an initial stage of mastitis, so any breast engorgement accompanied by an increase of body temperature should be considered as the serous stage of mastitis. Such an approach helps to start treatment in good time and thus prevent the process from moving into the suppurative phase of inflammation. If pyogenic microorganisms enter the breast with congestion, then after 2-4 days the breast becomes inflamed which sets the stage for the serous phase of mastitis. The condition is of sudden onset with a rise in body temperature, sweating, weakness, fatigue, and severe pain in the breast. The breast is found to be enlarged, tender on palpation, and the area of infiltration is not distinct. Milking is painful and does not bring any relief. Blood leucocytosis is up to 10-12x10", ESR up to 20-30 mm/hr. If treatment is delayed, the process can progress after 3-6 days to the infiltrative phase with pronounced clinical features of inflammation, and deterioration of the general condition. Temperature of the body may rise to 38-40 °C. The mass that is palpated assumes a more distinct form. The inflammatory process in the breast changes the milk acidity by increasing the pH of milk, which is due to the increase of the activity of alkaline phosphatase. Microscopic analysis of the cellular content of secretions from the breast shows large amounts of leucocytes. The transition of early forms of mastitis into purulent phase (fig. 90, colour inset) is characterized by an increase in intensity of both the local and general symptoms of inflammation. Body temperature is constantly high or hectic. Infiltration in the breast increases, as does the skin hyperemia, fluctuation appears in one of the breast segments. An abscess can be localized either superficially or deeper with a spread to the retromammary space (fig. 91).
Fig. 91. Topography of abscesses in mastitis: 1 - subcutaneous; 2 - intramammary; 3 - retromammary; 4 - galactophoritis. Patients with gangrenous mastitis are found to be critically sick: Body temperature is very high - up to 40-41 °C, pulse up to 120-130 beats per min, the breast is very swollen, skin is edematous with blisters containing hemorrhagic fluids and areas of necrosis. The edema spreads to the surrounding areas. High blood leucocytosis is noted with a shift to the left and toxic granular leucocytosis, protein is found in the urine. Mastitis can be complicated with the development of lymphangitis, lymphadenitis and rarely sepsis. After the abscess has burst, especially if it occurs spontaneously, a breast fistula that can close spontaneously after a long time may result. Treatment. Treatment of the initial stages of mastitis is conservative, and of the purulent forms - surgical. As soon as signs of breast congestion are noticed, the breasts should be supported in a raised position with either an immobilization bandage or brassiere that do not squeeze or press on the breasts but rather support them. Using a breast pump the breasts are evacuated of the milk; breastfeeding should be continued, fluid intake is limited, oxytoxin and nospani are given. Antibiotics are used in the case of serous and infiltrative mastitis (semisynthetic penicillins, aminoglycosides, cephalosporins, and macrolides), sulfanilamides (in combination with antibiotics), infusion therapy, including plasma substitutes, hemodes, protein preparations, saline solutions; substances that improve the body's resistance (gamma globulins, etc.) are also used. The breasts must be milked constantly to prevent congestion. A regression of the process can be enhanced by retromammal novocain block using antibiotics and proteolytic enzymes: 70-80 ml of 0, 5% solution of novocain, 500000 units of kanamycin and 10 mg of trypsin or chemotrypsin. To enhance a regression of the serous and infiltrative processes, ultraviolet irradiation, high-frequency-current therapy, ultrasonic therapy are used. All manipulations should be done after the breast has been emptied. In severe cases of mastitis it is recommended to suppress lactation by a combination of estrogen and androgen preparations. Purulent mastitis is an indication for surgery, which is done under general anesthesia; it is only in the case of superficially located small abscesses that surgery can be done under local anesthesia with retromammal novocain block. Wide and fairly deep incisions are made on the breast; all the pus and necrotic tissues are evacuated (fig. 92). Intramammary lesions are opened through radial incisions. After the pus has been evacuated, the cavity is examined using a finger, opening at the same time the various lacunae, hydrogen peroxide solution is used to wash or irrigate the cavity and the latter is dried. Then under adequate lighting the cavity is examined visually with the wound edges held open by retractors, while pressing on the breast. If it is found that some pus is entering the wound from a deeper area, then that opening is widened up to join the main cavity. All necrotic tissue lying loose in the abscess cavity is excised and removed. With several abscesses on the same breast, they are opened with separate incisions. Retromammal and deeplyseated intramammal abscesses are drained through semilunar incisions made through the lower inframammary fold. (fig. 93) In this way the breast is separated from the pectoralis major muscle. Intramammal abscesses are drained from their back, the cavity is drained and the resulting wound is sutured leaving the drainage site with the tubes. This method of incision and drainage prevents damage to the intralobular milk ducts while providing a good drainage of pus and necrotic tissues and at the same time giving a good cosmetic result. In localized forms of acute mastitis and especially in cases of chronic mastitis, the focus of infection can be excised within healthy tissue and firm sutures applied with a small drain inserted for the instillation of antibiotics. Treatment of the wound after incision and drainage is done taking into consideration the stage of the wound process. The use of secondary sutures cuts the healing time and improves the cosmetic results of the operation.
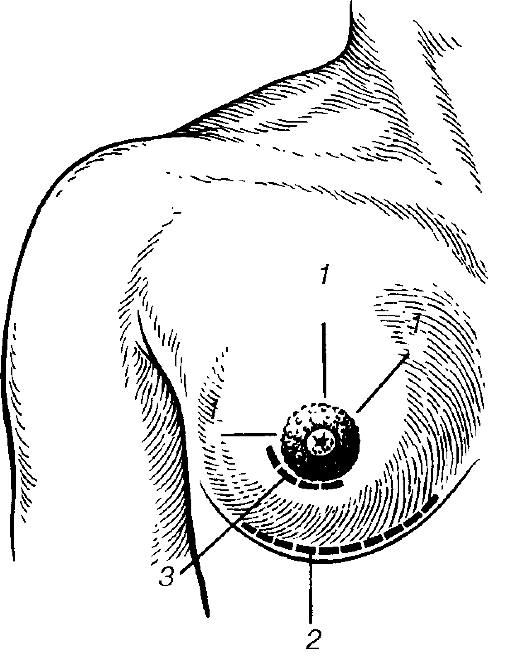
Fig. 92. Incisions made in suppurative mastitis: 1 - radial; 2 - Bardenheur's (incision); 3 - para-areolar.
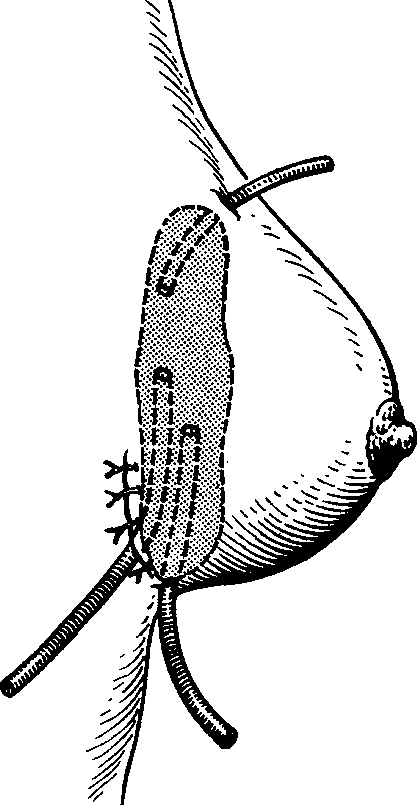
Fig. 93. Through and suction drainage in retromammary abscess. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 64; Нарушение авторского права страницы