|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
OSTEOMYELITIS AND ACUTE SUPPURATIVE ARTHRITIS
Osteomyelitis is an infectious disease characterized by the inflammation of bone tissue in which the pathological process involves not only the bone marrow but also the compact bony part, periosteum and often the surrounding soft tissues. Classification 1. According to their etiological factors: 1) nonspecific osteomyelitis; 2) specific osteomyelitis. 2. According to the mode of infection (transmission): 1) haematogenic; 2) non-haematogenic: a) traumatic; b) gunshot; c) contact. 3. According to the clinical manifestation: 1) haematogenic: a) acute (toxic form, septicopyemia, localizedform); b) primary chronic; c) secondary chronic; 2) non-haematogenic: a) acute; b) chronic. Two types of osteomyelitis are identified depending on the mode of penetration of the infection: haematogenic when an endogenic suppurative infection gains access to bone via the bloodstream, and Non-haematogenic when the infection reaches the bone from the outside (exogenic) (fig. 102). Non-haematogenic osteomyelitis occurs after open fractures, gunshots, internal fixation of bone (osteosynthesis) during healing of a fracture, in orthopedic operations, from the transfer of infection from the tissues surrounding the bone. Acute haematogenic osteomyelitis. Depending on the severity of the disease, the rate of development of the pathological process, the spread of infection, and other clinical factors three forms of acute haematogenic osteomyelitis are identified: toxic form, septicopyemia, localized form. Toxic form, which is often termed fulminant, is characterized by the development of extreme septic intoxication that starts in the early stage of the disease, the disease progresses rapidly and death ensues within the first few days. In this form the local pathological signs in the bone and its surrounding tissues do not have the time to develop. Septicophyaemic form, which is said to be severe, is characterized by the development of several suppurative-destructive foci in several bones simultaneously from the very onset of disease. Not infrequently abscesses are encountered in several parenchymatous organs such as the lungs, liver, and kidney. All this adversely affects the disease process leading to death in most instances. Bacteremia which is often encountered in this case contributes to the development of new osteomyelitis foci. Localized form of acute haematogenic osteomyelitis manifests itself as a mild form of infection compared to the two previous ones: symptoms of suppurative intoxication are mild and often associated with a single suppurative-destructive focus in the bone. Local signs of infection are more common than the general signs and intoxication. This type of osteomyelitis often develops into a chronic form. The toxic (fulminant) type is rare, the localized form of haematogenic osteomyelitis is the one commonly encountered. In the localized form the following local events occur as the process develops further: purulent exudate spreads along these two channels: through the bone marrow canal to the diaphysis of the bone and through the osteon canal (Haversian canal) - to the surface of bones. The periosteum becomes inflamed and most often pus is accumulated beneath it causing it to separate. Suppurative inflammation spreads to the surrounding tissues forming phlegmon, which later opens outside to form a fistula. Sometimes the surrounding tissue (paraosseal) phlegmon is accompanied by extensive and deep purulent accumulations that can open up as fistulas at sites far away from the affected bone. This is especially common for osteomyelitis of the pelvic bone, the vertebrae and the femur.
Fig. 102. The stages of osteomyelitis: a - haematogenous spread of infection; b - the primary focus; c - subperiosteal abscess; d - intercondylar phlegmon; e - subcutaneous abscess; f - osteomyelitic cavity with fistula; g - posttraumatic osteomyelitis. Because of the suppurative inflammation of the bone marrow, the periosteum and the involvement of the compact bone layers, blood supply to the bone is impaired and this leads to bone necrosis and the formation of sequestra. The extent of intoxication depends on the size of the primary focus of osteomyelitis, the amount of soft tissue involved in the process, the rate at which the purulent fistula opens up or the rate of surgical incision and drainage of the paraosseal phlegmon. Acute haematogenic osteomyelitis mostly affects children and young adults, and occurs 3-5 times more often in boys than in girls. The disease is of sudden onset but can sometimes be preceded by a feeling of general malaise 1-2 days before the onset. The patients with acute haematogenic osteomyelitis mostly complain of sudden onset of severe pain in the bone, often at the site of one of the major joints. The pain is felt as intense and throbbing. It is so agonizing that the patients cry, cannot sleep and the least movement in the affected bone may trigger intensive pain. They complain of malaise, headache, rise in body temperature, chills and loss of appetite. From the case history it is possible to establish the predisposing factors that could lead to the development of the disease such as limb contusion the past history of angina (acute tonsillitis), suppurative pharyngitis, the presence of tooth decay, pyogenic infections (furuncle, panaritium, infected wounds and abrasions etc.). All this can be the source of infection in the case of haematogenic osteomyelitis. During examination of the patient, signs of general intoxication are noted: weakness, adynamia, depression, sticky sweat, skin pallor, rapid breathing, tachycardia up to 110-120 beats per min. Heart sounds are dull with systolic murmurs. The spleen and liver are often enlarged; there is vomiting, paresis of the intestines, and renal pain with a positive sign of Pasternatsky. Examination of the patient in the first few days reveals a patient lying in a forced position with the affected limb in a bent position. Both active and passive movements in the adjacent to the affected area joints are strictly limited because of the extreme pain. To establish the focus of osteomyelitis gentle taps are done along the bone. Hitting on the heel may cause pain along the bone axis. The appearance of extreme pain in one of the meta-epiphysis is an indication of an acute suppurative inflammation in the bone. In later stages the skin over the affected bone becomes tense, indurated and then hyperemic. Palpation shows induration of the soft tissues, tenderness and local hyperthermia. Using a tape measure to measure the affected limb in comparison with the other healthy symmetric limb shows an increase in size of the affected limb due to the increasing oedema. In advanced stages of untreated acute haematogenic osteomyelitis local signs of phlegmon are elicited: swelling, skin hyperemia and fluctuation. Sometimes patients are admitted after the phlegmon has burst spontaneously on its own with the formation of fistula. In severe cases of osteomyelitis within 3-4 weeks after the onset of disease symptoms of pathological movements can be elicited in the affected limb, which is an indication of a pathological fracture occurring as a result of osteonecrosis. When the primary focus of osteomyelitis is located in the metaepiphyseal zone the adjacent joint is often involved in the inflammatory process. This is associated with typical signs of purulent arthritis: smoothening of the joint folds, fluctuation signs, limitations in the extent of movement, tenderness and the presence of purulent aspirate on diagnostic taps. These local symptoms are often sufficient to establish a diagnosis of acute haematogenic osteomyelitis. Difficulty in establishing the diagnosis occurs when the patient is admitted in the early stage of disease when the infection of the soft tissues has not yet developed. In such a situation, a diagnostic tap of the bone (osteoperforation) is indicated using a special needle in the corresponding metaphysis. The aspiration of a turbid liquid, pus or fluffy sanguineous content confirms the diagnosis of osteomyelitis. If unchanged blood is aspirated, the diagnosis of osteomyelitis has to be excluded but observation of the patient is continued. When the bone marrow canal is punctured, the patients with osteomyelitis, moreover, exhibit elevated bone marrow pressure of up to 300-400 mm of water level (normal values - 50 mm of H2O). Acute haematogenic osteomyelitis is associated with leucocytosis of up to 20x109/l with an increase in the number of neutrophils; ESR is always high. Hemoglobin is slightly low. Disproteinemia - low albumin levels and high levels of α 1 and α 2 globulins in the blood plasma - occurs at the same time. Urine changes are detected: traces of protein, leucocytes and cylinders. In the septicopyemic form of osteomyelitis bacteriuria is often disgnosed. Plausible X-ray signs of osteomyelitis appear not earlier than 10-14 days from the onset of the disease. From this time on it becomes possible to establish the thickening of periosteum, «erosion» of the bony architecture with the subsequent formation of cavity in the bone. The earliest but not constant sign of acute osteomyelitis on the X-ray is the increase in the soft tissue markings (shadows) adjacent to the damaged part of bone. Radionuclide and IR imaging techniques can be used to diagnose early forms of acute osteomyelitis. During the scintiscanning, hyperfixation of the pharmacological preparation to the affected bone segment can be identified on the 2nd-3rd day from the onset of disease. Data obtained by thermal infra-red imaging technique can also be used to establish the presence of infection in the bone and surrounding soft tissue within the first few days. Acute haematogenic osteomyelitis on many occasions has to be differentiated from rheumatism, the aftereffects of trauma, tuberculosis of the bone, bone destruction in the case of typhoid etc. To rule out traumatic injuries, the case history, the presence of general signs of inflammation and intoxication, X-ray data, laboratory findings etc. may be helpful. Rheumatism is associated with several days of prodromal period and the involvement of several minor joints whereas osteomyelitis affects as a matter of fact one joint. The effusion in rheumatism is serous and rather than purulent. In osteomyelitis the inflammation spreads to the metaphysis whereas in osteomyelitis it is limited around the epiphysis. Tuberculosis is associated with atrophy of the limb muscles and osteoporosis, radiographs show the features of a «melting sugar», whereas in osteomyelitis areas of osteoporosis are seen alternating with areas of osteosclerosis with the presence of cavities and in later stages - sequestra. Treatment. Therapy of acute haematogenic osteomyelitis is complex, a combination of surgical and conservative methods of treatment. In the presence of paraosseal phlegmon the latter has to be opened with the incision of the periosteum along the whole length of lesion and a trepanation of the bone. The operation is completed by wound drainage. It is important to properly immobilize the limb. The optimal surgical treatment is the early decompress drainage of the bone by way of drilling several holes in the area of osteomyelitis after incising the soft tissues. Drainage tubes are passed through the perforated holes into the purulent focus and active irrigation is effected in this way. Vacuum or long-term drainage with solutions of antiseptics (chlorhexidine, dioxidin, sodium hypochloride) conducted for at least 7-10 days and discontinued only when the suppuration has been eliminated and the patient's condition has improved is often used for this purpose. Extensive trepanation of the bone in acute haematogenic osteomyelitis is not recommended, since it creates the hazard of generalized infection - the development of septicopyemic metastasis in distant areas. Conservative therapeutic measures include antibiotic therapy, immune therapy, detoxication measures, the correction of metabolic disorders etc. It is good practice to use osteotropic substances (lincomycin, morphocycline, fusidin, gentamycin etc.) for the antibiotic therapy. The most effective administration of drugs is by intraosseous and regional (intraarterial, and intravenous) routes. Immunotherapy includes in the first place treatment by preparations for passive immunization (hyperimmune antistaphylococcal plasma, staphylococcal immunoglobulin), which is combined with staphylococcal anatoxin, bacteriophages, nonspecific immune therapy (prodigiozan, lizosim, methyluracyl etc) as well as desensitization preparations. Long-term fluid management depending on the indication includes: hemodes, reopolyglucan, protein blood substitutes, blood transfusion, albumin, protein, plasma etc. The successful treatment of acute haematogenic osteomyelitis depends to a large extent on how early the decompressive drainage of the bone marrow canal is done with the active aspiration by drainage of the focus of osteomyelitis. Chronic osteomyelitis. The condition is normally preceded by an acute form of disease. An exception is the rare case of primary chronic osteomyelitis of the following types: Garre's osteomyelitis, Ollier's osteomyelitis and Brodie's abscess. Osteomyelitis is divided into chronic, haematogenic and posttraumatic (gunshot, after nailing osteosynthesis etc.). The transition of osteomyelitis into the chronic form is due to several factors, most important of which are the late start of treatment, inadequate surgical procedures and wrong antibiotic therapy. The inadequate drainage of purulent foci favours the transition of the acute process into a chronic form. This often happens when the periosteum is not excised fully along its length and the openings made by drilling do not correspond to the spread of the process of osteomyelitis. The main fault of antibiotic therapy is using antibiotics without regard for the changing pattern of sensitivity of the pathogenic strains as well as the early termination of the antibiotic therapy for no apparent reason. The transfer of acute into chronic osteomyelitis is also determined by specific pathomorphological changes, complete expulsion of sequestra or the formation of osteomyelitic cavity at the site of osteolysis. The clinical presentation of chronic osteomyelitis comprises two phases: relapse and remission. Given active pathogenic strains and a body weakened by disease, exposure to radiation, injury and other factors, reactivation of the chronic process of osteomyelitis occurs - relapse of the disease. Under the effect of antimicrobial therapy or as a result of spontaneous healing of the active process, the whole condition may resolve and the phase of remission sets in. This kind of interchange of phases can be repeated several times. The following main triad of signs characterizes chronic osteomyelitis: relapsing trend, the formation of sequestra (or osteomyelitic cavity), purulent fistula. Relapse of chronic osteomyelitis presents as deterioration in the patient's general condition. The patient complains of general malaise, weakness, headache, rise in body temperature, sweating, chills. There is pain in the limb, and a purulent fistula opens up. In some instances the skin over the focus of osteomyelitis becomes hyperemic, intensive pain and induration of the soft tissue occur followed by the fluctuation sign and the old fistula that had closed early on opens up again, or a spontaneous opening of the phlegmon at a new site occurs. After the pus has been evacuated the patient's condition improves, intoxication reduces, temperature falls to subfebrile, local inflammation is gradually eliminated, the purulent fistula continues to function or also gradually closes up. The process enters into the remission phase, which can at any time change into relapse. The clinical presentations of the different kinds of chronic osteomyelitis are principally identical - there is an interchange of disease phases. In post-traumatic cases (including gunshot osteomyelitis), however, the area of bone infection is normally limited to the fracture site from whence the purulent fistulas emanate. Chronic haematogenic osteomyelitis is characterized by the presence of extensive areas of osteomyelitis along the metaepiphysis and diaphysis with the purulent fistulas, sometimes several of them, situated at different sites. Accordingly, the patient shows pronounced signs of chronic suppurative intoxication, changes in the blood picture (leucocytosis, increased ESR, disproteinemia), renal disorders, etc. When taking a history it is easy to elicit the previous episodes of an acute haematogenic osteomyelitis or a fracture of the bone that was complicated by suppurative process. The number of relapses should be ascertained, the duration of remission as well as the possible expulsion of minute bone sequestra from the fistula. The number of previous operations, their nature and the type of plastic that was applied to the bone cavity as well as the immediate postoperative outcome should be noted. Assessment of the patient's complaints should focus on whether the pains radiate to the joints, the presence of pain sensation along the vascular-nerve bundles, which can point to the development of new suppurative foci. The general symptoms of a relapse of chronic osteomyelitis are similar to those of any suppurative surgical disease, hence the body temperature is checked as well as the necessary blood tests and urinalysis are taken. In the presence of local signs the extent of skin hyperemia, soft tissue induration and the presence of signs of fluctuation are taken note of. It is important to assess the functional status of the fistula; a blunt probe is used to do the assessment, which in certain cases helps to establish the location of the focus of osteomyelitis. When an ulcer is found in the area of a long - standing purulent fistula, the edges and surface of the wound have to be thoroughly examined and if malignancy is suspected a biopsy is performed. To establish the extent of spread of the inflammatory process to the adjacent joint, the extent of movement, the presence of tenderness or effusion in it are assessed. X-ray methods help find out bone changes in acute osteomyelitis (periostitis or subperiosteal abscess) or chronic osteomyelitis (osteosclerosis, bone sequester or sequester box). Mild pathology may be detected by means of CT scan. Radiography is one of the most important diagnostic tools whereby the presence of sequestra, cavities, chronic periostitis is established and the extent of damage to the bone determined (fig. 103, colour inset). Fistulography is a very valuable method of investigation, it gives evidence of the direction of the fistula tract, its connection with the bone cavity, which is necessary in planning surgery, notably to determine the surgical approach (fig. 104). It is a must to investigate the type of pathogens and their sensitivity to antibiotics as well as the indications of specific and nonspecific immunobiological reactions of the body. Most often staphylococcal and gram negative strains either in monoculture or in association are identified and these are often resistant to a lot of antibiotics. Patients with chronic osteomyelitis are often found to have slightly lowered titers of staphylococcal antitoxin and indices of immunobiological reactions: complement titers, phagocyte activity, leucocytes, T-lymphocytes etc. Initially, primary chronic haematogenous osteomyelitis develops without marked inflammation. The following types of the disease are distinguished: 1. Brodie's abscess, or intraosseous abscess, i.e. a circumscribed necrosis of the bone sponge with its subsequent lysis and cavity formation. 2. Garre's disease, or severe sclerosing osteitis with areas of rarefaction in the bone and a spindle-shaped thickening of bone diaphyses. 3. Ollier's osteomyelitis, or albuminous osteomyelitis, i.e. slow accumulation of serous fluid rich in protein in the bone rather than of pus, which is occasionally followed by sequestration. Posttraumatic osteomyelitis results from traumatic bone fracture with subsequent local infection. Treatment. Surgical treatment for chronic osteomyelitis is indicated when there are sequestra, purulent fistula, osteomyelitic cavity in the bone, osteomyelitic ulcers, malignancy, in pseudoarthrosis, in cases of frequent relapse with severe pain, intoxication and dysfunction of the locomotive system as well as in the case of functional and morphological changes in the internal organs caused by the chronic suppurative infection. Contraindications to the performance of radical surgery - necrectomy - are severe renal failure associated with amyloidosis, decompensated cardiovascular and respiratory systems, etc. The main component in the complex treatment of chronic osteomyelitis (fig. 105, colour inset) is radical surgery - necrectomy, which is often referred to as sequestrectomy. The aim of the operation is elimination of the chronic focus of infection in the bone and its surrounding soft tissues. In radical necrectomy the sequestrum is removed, all osteomyelitic cavities are incised and liquidated together with their internal wall granulations and detritus; all purulent fistulas are excised. The next important step in the radical surgery is the sanitation and plasty of the bone cavity. More recently the plasty of bone cavity is achieved by using muscle pedicle flaps, bone plates (using autogenous or conserved bone tissue), chondroplasty (using conserved cartilage), and rarely, cutaneous flaps are used (fig. 106). Different biopolymer materials are used: collagen sponge impregnated with antibiotics, glue compositions with different ingredients and biopolymer plombes containing antiseptics. All these materials contain substances that enhance or activate bone tissue regeneration as well. Sanitation of the bone cavity after necrectomy is done by long - term methods of washing and drainage as well as vacuum drainage (fig. 107). These methods are sometimes used simultaneously: washing of the cavity is done through an afferent drainage tube with the efferent tube connected to a suction apparatus. In the case of washing drainage that is continued for 7-15 days different antiseptic solutions are used: antibiotics, dioxidin, soluble furagin, sodium hypochloride etc. The effectiveness of cavity sanitation is assessed and controlled by microbiological investigations. After necrectomy, treatment is aimed mainly at the suppression of the remaining microorganisms in the area of surgical manipulation, which yields a good immediate postoperative result.
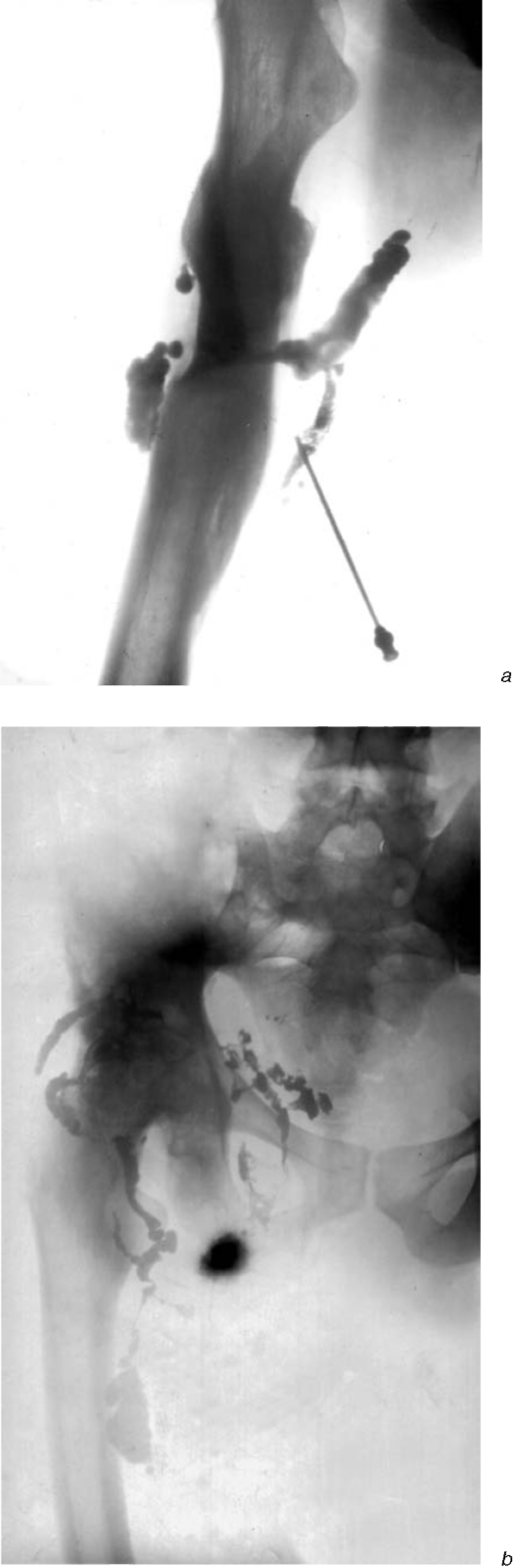
Fig. 104. Osteomyelitis: femoral (a) and iliac (b); fistular X-rays.
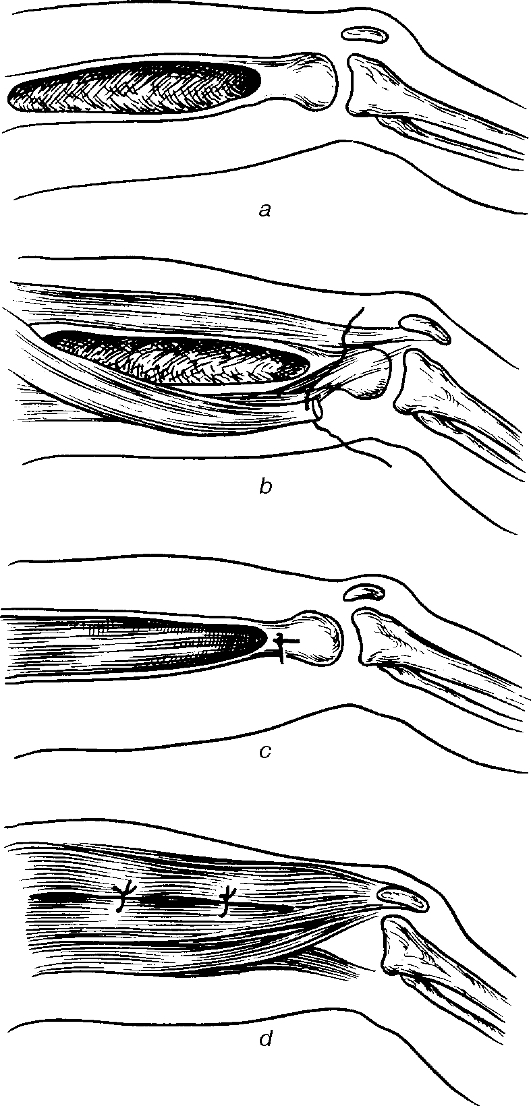
Fig. 106. Muscular plastics of the bone cavity for chronic haematogenous hip osteomyelitis: a - the bone cavity prepared for muscular plastics; b - the muscular flap on a proximal pedicle; c - the flap inserted in the bone cavity and sutured with the bone; d - periosteal and muscular suturing above the muscular flap. This aim is achieved by the following therapeutic measures: 1) antibiotic therapy, 2) immunotherapy, 3) local physiotherapeutic measures: ultrasound therapy, electrophoresis with drug preparations. Fluid management is initiated during the postoperative period: blood transfusions, protein blood substitutes, electrolyte solutions; correction of metabolic disorders; immobilization of the limb followed by exercise therapy to improve the functions of the locomotive system. Acute suppurative arthritis. This is an acute inflammation process of the joint caused by pyogenic microorganisms. Acute suppurative arthritis can either be primary or secondary. Primary contamination of the joint occurs with injuries to the joint; secondary infections occur when pathogenic pyogenic microorganisms gain entry to the joint by haematogenous spread from distant pyogenic foci or from purulent infected tissues surrounding the joint. Acute suppurative arthritis is often caused by staphylococcus. The changes that occur in the joint depend on the type of inflammation (serous, purulent, fibrinous or ichorous). The extent of spread of the process also plays an important role. The transition of the inflammation onto the joint cartilage and spongy tissue of the bone epiphysis suggests osteoarthritis and the inflammation of the surrounding soft tissue results in paraarticular phlegmon (fig. 108, 109). The clinical presentations of acute suppurative arthritis are: sudden onset, severe pain and limitations in the joint movement, tension, induration and hyperemia of the integument as well as a change in the joint size and shape. In complicated cases local signs of phlegmon are encountered. General clinical symptoms include the presence of suppurative intoxication: high body temperature, weakness, malaise, chills, sweating, depression, progressive anemia etc.
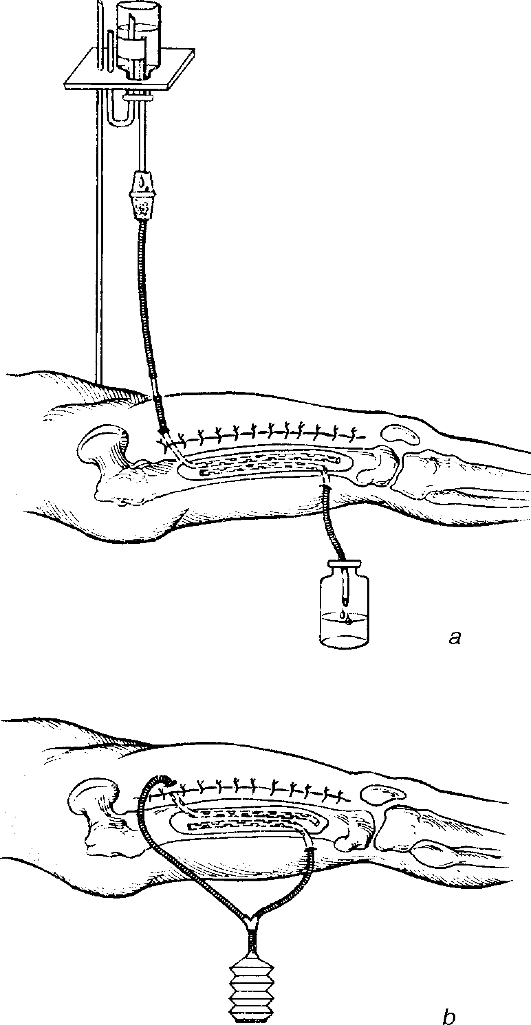
Fig. 107. Post surgery bone cavity drainage in chronic femoral osteomyelitis: a - through; b - suction.
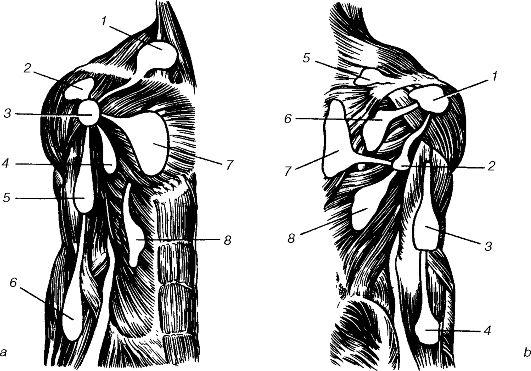
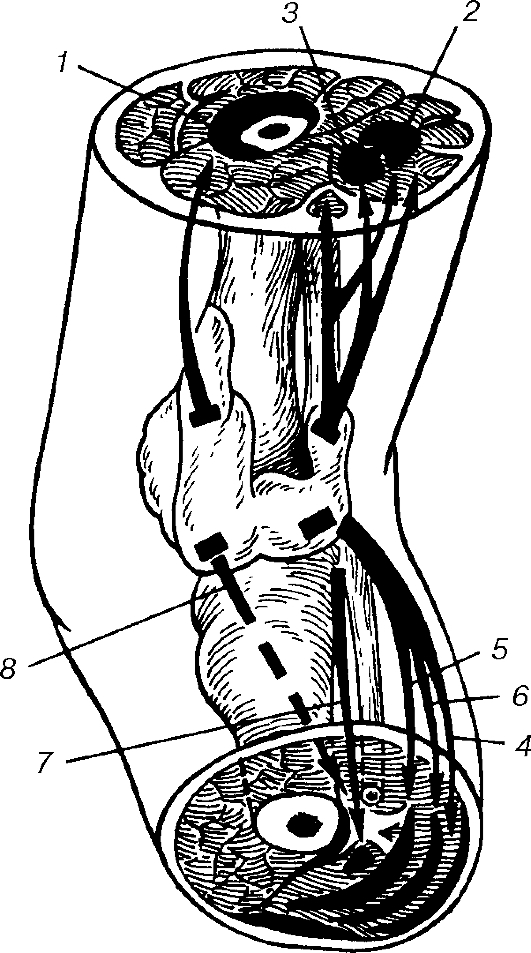
Fig. 108. Topography of humeral suppurative arthritis: a - anterior surface: 1 - supraclavicular; 2 - subdeltoid; 3 -arthral; 4 - axillary; 5- anterior humeral; 6 - anterior forearm; 7 - subpectoral; 8 - abdominal wall; b - posterior surface: 1 - subdeltoid; 2 - axillary; 3 - posterior humeral; 4 - posterior forearm; 5 - supraosteal; 6 - subspinal; 7 -subtrapezoid; 8 - sublatissimus dorsi. Examination of the patient with acute suppurative arthritis has its peculiarities. When taking history the presence of injuries to the joint should be elicited. The absence of the history of trauma suggests the haematogenic way of infection. Inspection should focus on half-bent forced position of joint, hyperemia of the skin and the extent of distortion of the joint configuration. The affected joint has to be compared to the symmetrical healthy one. Palpation shows a higher temperature over the affected joint, tenderness, fluctuation, which indicates the accumulation of fluid in the joint space or the presence of paraarticular phlegmon. With large amounts of fluid accumulated in the knee joint, the patella is found to be floating. The extent of motion in the affected joint has to be assessed. The extent of limitations in the affected joint is an indirect indication of the severity of the inflammatory process. Blood tests show the usual signs of suppurative inflammation: leucocytosis, neutrophilia, high ESR and disproteinemia. X-ray in acute suppurative arthritis shows a widening of the joint spaces, osteoporosis at the epiphyseal bone ends of the affected joint. Puncture or a tap of the joint is crucial: the aspirate can be used to identify the type of inflammation (serous, purulent, purulo-hemorrhagic etc.). The aspirated fluid is sent for microbiological investigations to determine the type of pathogenic microorganisms and their sensitivity to antibiotics. Treatment. Treatment of acute suppurative arthritis combines both local and general therapeutic measures. Local measures include: a) puncture of the joint with aspiration of its contents, irrigation or washing of the joint cavity with antiseptic followed by infusion of antibiotics (fig. 110). Therapeutic punctures are done daily until the accumulation of inflammatory exudates into the joint has stopped; b) immobilization of the joint with either POP slab or a therapeutic splint; c) physiotherapy: high-frequency therapy, quartz irradiation, electrophoresis with trypsin, antibiotics etc.; d) after the inflammation has subsided the patient is prescribed exercise therapy, massage and other manipulations to restore the joint functions.
Fig. 109. Topography of suppurative gonitis: 1 - deep superior anterior; 2, 3 - superior posterior; 4 - inferior superior posterior, between the gastrocnemius and sole-us muscles; 5 - inferior posterior, under the deeper layer of the crural fascia; 6 - between the soleus muscle and the deeper layer of the crural fascia; 7 - the posterior surface of the interosseous membrane; 8 - inferior posterior, along the interosseous membrane. General therapeutic measures include antibiotic therapy tailored to the results of microbiological investigations, immunotherapy, blood transfusion, plasma, protein blood substitutes, detoxication therapy, rational nutrition rich in protein and vitamins. Surgical treatment involves arthrotomy, which is indicated only where the puncture and aspiration, local and general antibiotic therapy prove unsuccessful. During arthrotomy the joint cavity is cleared of all the purulent effusion and fibrinous deposit whereupon a drainage tube is placed for long-term washing sanitation (fig. 111). Paraarticular phlegmon has to be incised and drained followed by subsequent treatment along the standard lines.
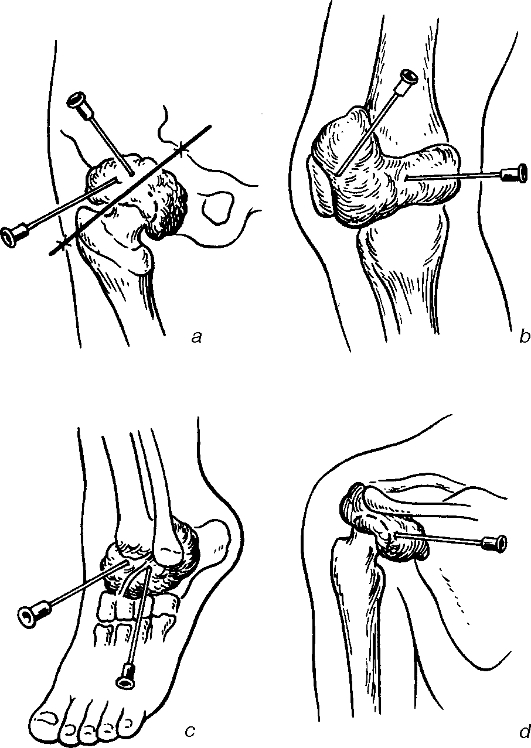
Fig. 110. Arthrocentesis in suppuration of the hip (a), knee (b), ankle (c) and shoulder (d) joints.
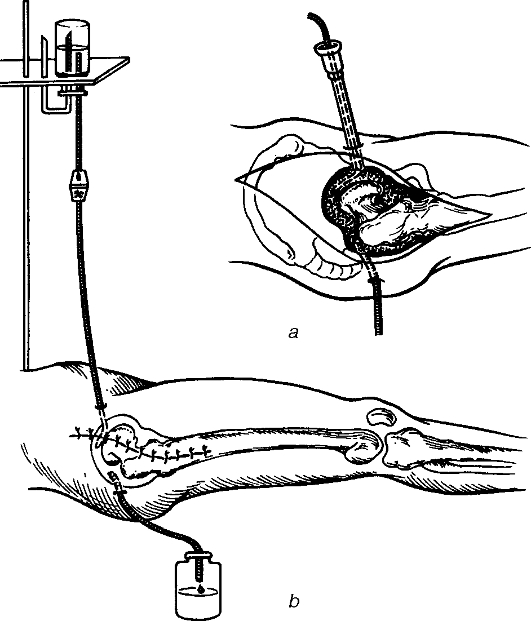
Fig. 111. Through drainage of the hip joint after arthrotomy: a - arthrocentesis followed by insertion of the microirrigator; b - through drainage of the hip joint with antibiotics. Prophylaxis of acute suppurative arthritis involves a thorough execution of the primary surgical wound debridement, especially when the joint is affected, strict compliance with aseptic measures during orthopedic operations and correct treatment of suppurative inflammations of contiguous tissues (abscess, phlegmon, osteomyelitis, furuncle etc.). ACUTE THROMBOPHLEBITIS This is an inflammation of the vein concurrently with the formation of thrombus. Two types of processes are identified: phlebothrombosis - thrombosis developing as a result of blood stasis and changes in the blood clotting system, and thrombophlebitis - thrombosis developing on the background of inflammatory changes in the walls of the vein. Factors that cause the development of the disease have to be elicited during examination of the patient: 1) blood stasis (reduction of the rate of blood flow); 2) changes in the blood composition; 3) damage to the vascular intimae. Such conditions are encountered during surgical manipulations especially in women - in diseases of the uterus, operations on the kidneys, and urinary tract and during femoral neck fractures. Venous stasis and the reduction of blood flow may occur when patients are immobile, in cardiac failures, and in pregnancy. The source of infection can be acute or chronic infections (typhoid, pneumonia, influenza, septicemia etc.). Damage to the vascular intimae occurs during trauma (fractures, contusions, haematoma, crush, immobilization and catheterization of vessels). Changes in the blood composition occur in diseases of the blood (anemia, leukemia etc.), treatment with certain types of drugs (digitalis, mercury containing diuretics, vitamin K, corticoids and antibiotics, especially penicillins). Acute superficial thrombophlebitis. This kind of thrombophlebitis is often easy to diagnose. Patients complain of pains, infiltration and tenderness along the affected vein. Pains intensify on walking as well as during active and passive motions. Varicose-enlarged veins of the leg and thigh are often affected. The body temperature rises, and inspection of the limb shows a firm infiltrate along the vein that is tender on palpation. The skin is hyperemic and edematous (fig. 112, colour inset). When intact veins are affected especially in obese patients a firm tender threadlike induration is palpated along the vein. Treatment. Conservative therapy in the acute stage of the disease when the patient is febrile includes rest with the limb raised, anti-inflammatory and anticoagulant therapy (acetyl salicylic acid, butadion, rheopirin, venoruton, troxevasin; compress with heparin, venoruton ointments, novocain block with heparin), physiotherapeutic measures (electrophoresis with trypsin, potassium iodide, soluxe, high-frequency current therapy); minimum walking exercise with the limb bandaged with an elastic bandage. Indications for surgery (absolute and relative) are when the thrombus is situated at the ostium of the superficial vein (the danger of the process extending into the deep veins and thromboembolism); suppurative thrombophlebitis (the danger of sepsis). The thrombosed vein is excised or ligated at the point of entry into the deep vein. Thrombophlebitis of the deep veins. This condition is more serious than the superficial one. Patients mainly complain of pains and oedema of the limb. Pain is spontaneous and varies in intensity and character: in thrombosis of the deep veins of the leg the pain is localized in the calf muscles and tends to increase on walking; in thrombosis of the deep veins of the thigh or in ileofemoral thrombosis as a result of the rapidly developing oedema the pain is severe and throbbing. In ileofemoral thrombosis the patient's general condition deteriorates as a result of the intoxication: the patient becomes weak, there may be tachycardia, fast respiratory rate, dullness in the heart sounds. Examination of the limb reveals oedema, the location of which depends on the spread and site of thrombosis: oedema of the ankles is characteristic of thrombosis of the popliteal veins; oedema stretching to the knee is characteristic of thrombosis of the common femoral vein; oedema of the thigh occurs in thrombosis of the femoral and iliac veins; oedema of the legs and the abdominal wall - in thrombosis of the inferior vena cava. Oedema is most pronounced in thrombosis of the femoral and iliac veins. It presents in two forms: a) phlegmasia alba dolens - white shiny skin, smooth, waxy, oedema is firm, no mark is left on the skin when it is pressed down with the finger; b) phlegmasia coerulea dolens - bluish skin, spotty, moist, shiny with a reduced skin temperature. Oedema is found early in the course of disease when the patient is standing but it increases very fast and is associated with extreme intoxication. Pulsation on the peripheral arteries is absent. In thrombophlebitis of the deep veins of the leg, palpation of the calf muscles reveals tenderness along the deep veins, pains in the calf muscle appear on dorsal flexion of the foot or 5 minutes after the pressure in the blood pressure cuff has been increased to 40 mm Hg. Pains are felt at the site of thrombosis on coughing, sneezing or tapping on the anterior surface of the tibia bone. Treatment. Bed rest with the leg raised, anticoagulants and fibrinolitic therapy (heparin injections, fibrinolysin, streptase, streptokinase, urokinase), followed by indirect anticoagulants (neodicumarin, pelentan, phenylinum etc.). At the same time preparations that improve the rheologic properties of blood are prescribed (reopolyglucin, hemodes, trental and nicotinic acid). Surgical treatment includes thromboectomy, ligation of the vein, autovenous shunts and prosthesis after resection of the vein with the thrombus, plication of the vein, the implantation of filters into the vena cava inferior as a prophylactic measure against thromboembolism of the pulmonary arteries. In thrombosis there is always the possibility of the superficial process spreading to the deep veins (through the ostium of the superficial or communicant veins), embolism of the pulmonary arteries, further progression (spread to other organs). Deep vein thrombosis often leads to the development of post-thrombophlebitis disease. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 128; Нарушение авторского права страницы