|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Chapter XII. TUBERCULOSIS OF BONES AND JOINTS
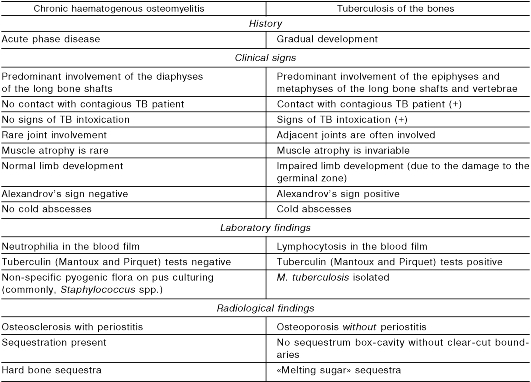
Caused by Mycobacterium tuberculosis, tuberculosis (TB) most commonly affects the lungs, lymph nodes and serous membranes, the bones and joints being the last to be involved with the incidence as low as about 10%. The major sites of osseous and articular tuberculous lesions include the epiphyses of the long bone shafts, bodies of the short bones: f.e. vertebrae and diaphyses of the digital phalanges. Anatomically, this type of tuberculosis falls into three major forms: • tuberculous spondylitis, or spinal TB (40%); • tuberculous coxitis, or hip joint TB (20%); • tuberculous gonitis, or knee joint TB (15-20%). Tuberculosis of the bones and joints is usually due to a secondary TB infection, which implies its lymphohaematogenous spread from the primary pulmonary focus or that of other organs. M. tuberculosis bacteria induce specific inflammatory reaction within the bone marrow of epiphyses, the site known to have a slower blood flow. This results in primary ostiitis, or tuberculous osteomyelitis. The initial tuberculous focus undergoes caseous («cheese-like») necrosis around which further tubercles form to merge with the initial focus. Subsequently, granulation occurs which, in turn, is subject to necrosis. This leads to sequestration: the bony tissues involved in the necrosis become completely separated from the underlying bone. The progression of tuberculous inflammation into the joint forms an articular sac with subsequent caseous necrosis of the joint cartilage and contiguous osseous tissues. Primary synovial tuberculosis (TB synoviitis) only occurs in about 5% of cases, with a favourable outcome as it is unlikely to cause the damage to the joint ends of the bones. According to P.G. Kornev, the pathogenesis of tuberculosis of the bones and joints involves the three stages: stage 1 - pre-arthritis-formation of the bone focus in the epiphysis around the joint; stage 2 - arthritis - extension of the process to the joint with resultant secondary arthritis; stage 3 - post-arthritis- stabilisation of the disease with the evidence of its complications. Therefore, to distinguish the pathological stage is of practical importance for the identification of the clinical picture and deciding on the therapeutic strategies. Examination of the patient A. History 1. Complaints • loss of appetite; • easy fatigability; • difficult walking; • weight loss; • low grade fever. 2. History of present illness • impaired limb function followed by pain on moving (most often in the back, hip and knee joints) which, as a rule, worsens on walking and bending. 3. Family and past medical history • evidence of tuberculosis in the family (e.g. parents); • contacts with contagious tuberculosis cases; • provoking factors (e.g. trauma); • history of an infection. B. Physical examination • weight loss; • muscle atrophy at the limb affected; • skin and mucosal pallor. C. X-ray of bones (to detect changes in the spongy bone tissues at metaphyses): • osteoporosis; • foci of sequestration coupled with clear areas in the form of a soft shadow («a piece of melting sugar» sign); • widening of the joint space followed by its narrowing; • notching of joint cartilaginous and osseous tissues; • osteosclerosis and periostitis are usually absent. It is noteworthy that tuberculosis of the bones has to be differentiated from chronic haematogenous osteomyelitis (see tab. 8). Tuberculous spondylitis A. Epidemiology • the vertebrae are the most common site for bone-joint tuberculosis; • children in their early years are primarily affected; • vertebrae Th2 - 4 are usually involved. Table 8. Chronic haematogenous osteomyelitis vs tuberculosis of the bones: differential diagnosis
B. The clinical picture (depends on the phase of the disease process). Stage 1 - prespondylolytic - the inflammation is confined to the vertebral body: • symptoms and signs of tuberculous intoxication (anorexia, weight loss, misbehaviour) without clinical signs of vertebral involvement; • laboratory findings indicative of active TB; • mantoux test positive; • lymphocytosis; • high ESR; • spinal X-ray films (of importance! ); • the foci of osteoporosis and destruction in the vertebral bodies. Stage 2 - spondylolytic - destruction of the vertebral bodies with the process spreading to the intervertebral disks and the contiguous tissues • symptoms and signs of tuberculous intoxication; • pain on bending and limitations in the spinal mobility (the child is unable to pick up things while standing and has to squat); • Inspection of the spine shows; • distorted spine with the spinal processes jolting out and gibbus; • «reins» sign (tension of the back muscles on unbending); • «a piano key» sign (pain on palpating the prominent spinal processes). Cold abscesses and purulent fistulae appear at this phase, and a shift in the vertebra can lead to compression of the spinal cord and paralysis of the limbs, impaired micturition and defecation (fig. 123).
Fig. 123. Wandering abscesses in tuberculous spondylitis. X-ray films show flattening the vertebral bodies, which is a sign of their destruction due to pathological compression fracture, a shadow of the stretching cold abscesses can be noted. Stage 3 - postspondylolytic- is characterized by the subsiding of the inflammation. The cold abscesses, fistulae and impaired spinal innervation can still persist. Tuberculous coxitis A. Epidemiology. • Tuberculous coxitis accounts for about 20% of all cases of bone and joint tuberculosis. • Children of 3-7 years of age are most commonly affected: B. Clinical picture. • symptoms and signs of tuberculous intoxication; • pain at the hip joint irradiating to the knee joints and getting worse on walking (which forces the child to assume the position with his/her thighs bent up as the relaxation of the joint capsule alleviates the pain); • muscle atrophy; • smoothened inguinal and gluteal folds; • purulent fistulae. X-ray pictures show narrowed joint spaces, severe osteoporosis, destruction of the femoral head or the gluteal cavity. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 71; Нарушение авторского права страницы