|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Transportation immobilisation
Providing immobility and rest for an organ, part of or the whole body during transportation of the patient to a surgical centre is termed transportation immobilisation. The aim of the transportation immobilisation is to prevent extra tissue and organ damage, development of shock during moving the patient and transportation. Indications for the use of transportation immobilisation are bone fractures, injuries to the joints, major vessels, nerve trunks, extensive wounds, crushed extremities as well as infections of the limbs (acute osteomyelitis, acute thrombophlebitis). The following are the main rules and regulations of transportation immobilisation: • Immobilisation has to be done at the accident site, moving the injured person without first immobilising is not allowed. • The patient has to be given analgesia (promedol, morphine) before immobilisation is started. • Bleeding has to be stopped first by applying a tourniquet or some pressure dressing; an aseptic dressing is put on the wound. • The splint is applied right to the clothing, if, however, the splint has to be applied to the bare skin, some cotton wool or napkin or the patient's clothes should be placed on the skin before the splint is applied. • Two joints adjacent to the injured one are to be immobilised in extremity injury; if it involves the thigh, all the three lower limb joints are to be immobilised. • In closed fractures, the extremity is slightly pulled along its axis during splint application, holding on to the distal part of the arm or leg and fastened in that position. • In open fractures pulling is not allowed; the limb is fastened in the position in which it is found. • If a tourniquet has been applied to the extremity before the splint, it must be seen to it that the splint bandage does not cover the tourniquet. • In moving the injured person after immobilisation the assistant has to support the injured part. In inappropriate immobilisation, the displacement of bone fragments during transportation and movement of the patient can turn a closed fracture into an open one. Also, mobile fragments can cause damage to the vital organs - major vessels, nerves, brain and spinal cord, thoracic, abdominal and pelvic organs. Extra injuries to the adjacent tissues can lead to shock. For transportation immobilisation, standard splints (Kramer's, Dieterich's, pneumatic splints), vacuum immobilisation stretchers as well as plastic splints are used. Kramer's ladder splint is universal. This kind of splint can be transformed to acquire whatever desired configuration desired. More variants are made by joining several Kramer's splints together. They are used to immobilise the upper and lower limbs and the head. Dieterich's splint consists of movable outer and inner plates, plywood bases with metal brackets. This type of splint is used for fractures of the femur, pelvis and the knee joint. The advantage of this splint is that it serves to combine immobilisation with traction. Inflatable splints comprise a double layer of airtight soft case with a closing zip. The soft case is put on the limb, the zip closed and air pumped into it through a tube, to make it firm. To remove the splint the air in it is allowed to escape and the zip opened up. This type of splint is simple and convenient, and transparent for X-rays. The splint is used for immobilisation of fractures of the hand, forearm, elbow joint, the foot, shin and the knee joint. In the absence of commercial splints, they are made of available materials ex tempore: a board, ski, stick, or a door (for the transportation of patients with spinal injuries). The standard Yelansky's plywood splint is used to immobilise patients with injuries to the head and the cervical spine (fig. 46). The splint folds are opened, cotton wool layers are placed over the side with the semicircular oilcloth bolster cloth to support the head. The splint is applied beneath the head and the upper part of the chest and fastened with belts to the trunk. The head is placed on a special hollow for the occipital region and is bandaged to the splint.
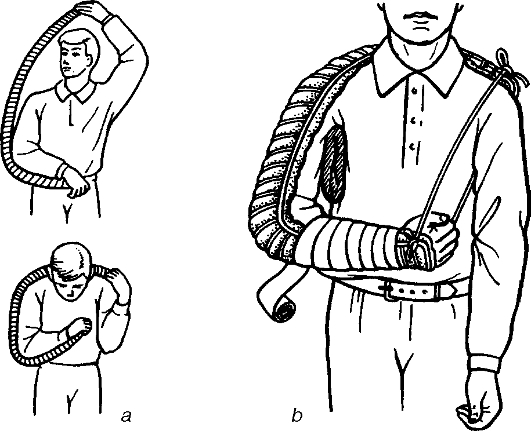
Fig. 46. Transportation immobilisation of the head and cervical spine using the Yelansky's splint. To immobilise the head, a cotton wool, or gauze ring can be used. The injured person is put on the stretcher, the head placed on the cotton wool ring in such a way that the occiput is fitted in the hollow of the ring. The patient is then tied to the stretcher to prevent him/her from moving during transportation. Cotton wool and gauze collars of the Shants type are used to immobilise patients with neck injuries like the if the patient is neither vomiting nor has difficulty breathing. Three to four layers of cotton wool are bandaged around the neck to form the collar, its upper part supporting the occiput and the mastoid processes, and the lower ones resting on the chest (fig. 47). Immobilisation of the head and neck can be achieved by the application of the Kramer's splints that have been preliminary bent to fit the shape of the head. One splint is placed under the head and neck, the other one is folded into a semicircle, the ends of which press against the shoulders. The splint is then fastened with a bandage. In case of a fracture of the clavicle, the fragments are immobilised with Desault's bandage, or a triangular bandage with a bolster placed in the armpit or with a figure of 8 bandage (see «Dressings»). Fractures of the humerus and injuries to the shoulder and elbow joints can be immobilised by the application of a large ladder Kramer's splint that has been preliminary moulded on the physician (fig. 48). The limb is positioned as shown in the Figure with a bolster placed in the armpit. The splint fastens all the three joints of the upper limb. The upper and lower ends of the splint are secured with a tape of bandage, one end of which has been passed in front and the other under the armpit on the intact side. The lower end of the splint is hung on the neck using a belt or scarf.
Fig. 47. Cotton-and-gauze collar for transportation of the patients with cervical damage.
Fig. 48. Immobilisation of the upper limb using a ladder splint: a - modelling Cramer's splint; b - view after application of Cramer's splint. In the absence of standard splints, fractures of the shoulder or humerus in the upper third can be immobilised to make up a triangular bandage. A small cotton wool-gauze bolster is put in the axilla and bandaged to the chest through the intact shoulder. The arm, which is bent in the elbow joint at 600, is hung on the triangular bandage, the arm is then bandaged to the body. For the immobilisation of the hand and forearm a small ladder splint is used, onto which the hand and forearm are bandaged fastening the wrist and elbow joints. The arm is bent in the elbow joint and the hand after the application of the splint is hung on the scarf. In the absence of special splints the forearm can be hung on a scarf or immobilised with a board, carton, plywood with fixation of two joints as a must. In femoral rod fractures, and those of the hip and knee joints, the Dieterich's splint is applied. The foot end of the splint is bandaged to the sole of the patient's shoe using a figure of 8 bandage. The external and internal plates of the splint are adjusted to the injured person's height by shifting the bracelets and fastening them by pins. The external plate is pushed to support against the armpit, and the internal plank in the inguinal region, the lower ends should appear beneath the sole for about 10-12 cm. The plate is passed through the cramp of the sole plate and stuck together with a collar. A string is passed through the hole in the sole and tied together on the screw stick. Several cotton wool-gauze pads are put on the ankle joints and on the plate of the clutches. The splint is fastened to the body with bandages and the planks are fastened to each other. The leg is pulled beyond the sole plates (fig. 49) and the screw board is screwed. The splint is bandaged to the leg and body. On the posterior aspects of the leg the Cramer's splint is placed and bandaged to prevent the leg form falling backwards. For immobilisation of the injured, thigh Cramer's splints (fig. 50), which have been fastened to each other can be used, they are placed on the lateral, medial and posterior aspects. It is a must to immobilise the three joints. Fractures of legs are immobilised with the Cramer's splint. Fixation is achieved by using three splints; making in that way the knee and ankle joints immobile. The shin and knee joints are immobilised with the inflatable splint (fig. 51).
Fig. 49. Application of the Dieterichs' splint: a - plantar fixation; b - limb traction in the splint; c - the view of the splint applied.
Fig. 50. Transportation immobilisation of the lower limbs using the ladder (Cramer's) splint.
Fig. 51. Medical pneumatic splints: a - for the hand and forearm; b - for the foot and shin; c - for the knee joint. In fractures of the pelvic bones the injured person is transported on a stretcher, a wooden board or plywood plate has to be put under it. The legs should be flexed in the hip joints, with some pads of cloth or pillow placed under the knees (fig. 52). The injured person is then tied up to the stretcher. In fractures of the spine in the thoracic and lumbar regions, the injured person is transported on a stretcher with a board. The patient is placed supine with pads of cloth or pillow placed under the knees. The injured person is then tied up to the stretcher. In case the patient has to be transported on a soft stretcher he/she is made to lie on the stomach with some pad under the chest. In trauma to the neck and upper thoracic spines, the injured person is transported lying supine on a stretcher with a pad under the neck. In severe injuries to the spine, pelvis, and severe multiple injuries, transportation immobilisation is done with vacuum immobilisation stretchers (VIS). The injured person is placed on a double airtight case on which and the mattress laced up. Vacuum of 500 mm Hg is created in the case using a vacuum absorber. It takes about 8 minutes for the mattress to get firm due to cohesion of polyester foam granules contained in it, which constitute 2/3 of the volume. The patient is placed to assume the position required for transportation (e.g. half sitting position) during filling with vacuum (fig. 53).
Fig. 52. Transportation of the injured with the spinal fracture using the board.
Fig. 53. Vacuum immobilisation stretcher: a - general view; b - stretcher with the patient lying inside; c - stretcher with the patient in a half-sitting position. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 736; Нарушение авторского права страницы