|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Classification of gas gangrene
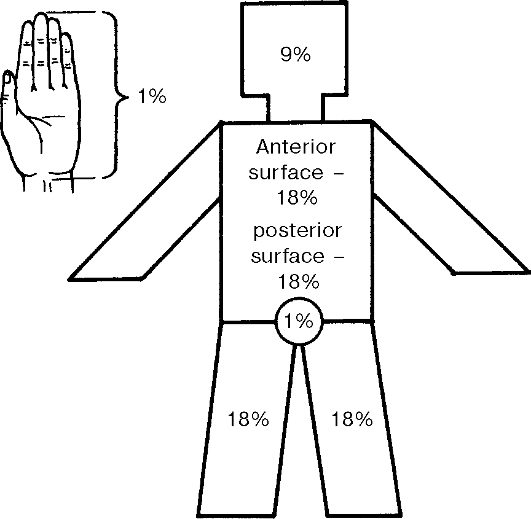
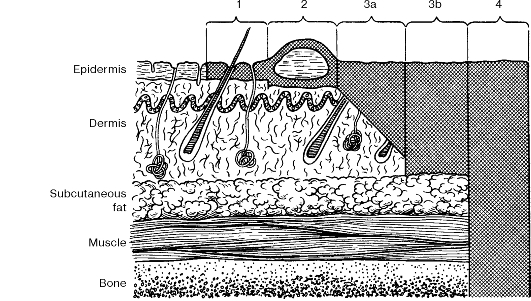
1. Localisation: • Clostridial myositis. • Clostridial cellulitis. 2. Clinical course: • Fulminant. • Fast progressive. • Slow progressive. The incubation period for gas gangrene lasts 1-3 days; in fulminant forms, however, it can only take a few hours. The earlier the infection sets in, the more severe it is. Factors that predispose to gas gangrene are as follows: • injuries to the lower limb with concurrent massive tissue damage, tissue contusion and marked contamination of the wound with soil, clothing etc.; • blood circulatory disorders due to the injury; • ligation of major blood vessels; • vascular occlusion by the applied tourniquet; • tight bandaging; • lowered general body resistance due to shock, anaemia, frostbite, long starvation periods, vitamin deficiencies, and secondary trauma resulting from inadequate transportation and immobilisation). Early signs of anaerobic infections include the following: — the patient's inadequate behaviour (e.g. restlessness, agitation or adynamia); — fever; — tachycardia; — pain in the wound, pains and tenderness along the vascular-nerve bundles of the affected limb, a sensation of tightness at the bandage. Examination of the wound can show a change in the wound discharge, eventration of muscles into the wound, oedematous wound edges, and the appearance of blisters on the skin. Specially placed tight control bandage leaves a mark on the skin after removal and the sutures seem to be «cutting through» the skin. Deep pressing with fingers does not leave fingerprints on the oedematous tissues. The presence of oedema is confirmed by the clearly distinct deepening of hair roots on the skin. Oedema spreads to a particular limb segment or the whole limb. The presence of gas (a «crepitation» sign) on palpation of the tissues confirms the diagnosis. Shaving of the skin around the wound gives a typical high metal sound (a «shave» sign). The formation of gas usually starts from the deeper tissues, which affects its elicitation at early stages. In such cases X-ray investigations can show the presence of gas. Serial examinations can confirm the increasing oedema. X-ray shows radioluscent areas around the bones, and in between the muscle bundles because of accumulation of gas in those areas. Such signs as pain, fever, and an increase in the limb's size require that the urgent wound revision be done. Slow progression of anaerobic infections is characteristic of a localized injury signs. The infection develops gradually, the pain is mild and intoxication is moderate, gas accumulates around the wound, wound discharge is serous and purulent with an offensive odour. This kind of localised anaerobic infection is known as clostridial cellulitis. In fast developing fulminant forms of gas gangrene, the incubation period lasts from a few hours up to 2 days. Then oedema of the limb develops rapidly, the skin gets stretched and skin folds disappear. The skin of the affected limb becomes pale and icteric with bronze-greenish-blue patches. The epidermis exfoliates in blisters with transparent or turbid contents. Gas accumulates in the subcutaneous tissues and muscles. Grey muscles can be seen in the wound. Intoxication worsens fast. This type of anaerobic infection is termed asclostridial necrotising myositis. The causes of fulminant development of the infection are not fully understood. Clostridial necrotising myositis is not so common as clostridial cellulitis and not infrequently leads to amputation of the affected limb. Inspection of the wound reveals swollen muscles that are first «waxy» and then appear as boiled meat. Dirty grey film may cover the wound. On pressing on the wound edges, gas bubbles appear. The granulation is absent and the wound discharge of light yellow to dirty brown colour is scanty and is occasionally jelly-like. When putrid infection develops in addition to gangrene, a smell of rotten tissue can be noted. Qualitative and quantitative changes of the exudate and dryness of tissues imply poor prognosis. An increased serous secretion suggests the subsiding of the process. The appearance of thick pus discharge implies the presence of a secondary purulent infection. Oedematous wound edges with hyperaemic surrounding skin are typical of severe secondary purulent infection. Gram stain of the wound smears can confirm the diagnosis if large gram-positive bacilli are revealed. Cultural studies, however, are of limited value in the acute period of infection but their results can be very helpful for the subsequent adjustment of antibiotic therapy. Complex prevention of anaerobic infection includes early first aid to injured persons, prevention and treatment of shock, anaemia as well as early primary surgical wound debridement. Primary surgical wound debridement should be preceded by complete excision of necrotised tissue, opening of pockets of pus. Gunshot and crushed wounds are not to be sutured. Thorough immobilisation of the limb, both transportation and therapeutic is important. In extensive injuries or severe contamination, polyvalent antigangrene serum is given to prevent infection. The average prophylactic dose of serum is 30, 000 IU (10, 000 IU for each of the three main causative agents - Cl. perfringes, Cl. oedematiens, Cl. septicum). Treatment should be started as early as possible. The patient should be isolated into special cubicles. Emergency operation is indicated which includes incision of the wound and removal of necrotic tissues, especially muscles. In severe advanced cases, the limb has to be amputated (without using a tourniquet or suturing). In critical cases, amputation with extensive tissue excision and fasciotomy of the stump is done without suturing the wound. Following surgery, wounds need to be treated with antiseptics such as oxidants (e.g. hydrogen peroxide, potassium permanganate). The indications for limb amputations are as follows. • Gangrene of a whole segment of limb. • Progression of the process despite previous primary wound debridement (primary surgical debridement, stripe incisions) and provision of complex therapeutic measures. • Severe gunshot injury leading to extensive damage to the bones and joint of the limb. • Ischaemia of the limb following irreversible damage to the major vessels. Fractured limb must be immobilised by using skeletal traction, plaster bars (the application of circular POP bandages is contraindicated in these cases). Specific treatment should be started immediately. During the operation, intravenous infusion of serum at a rate of one ml/minute is given under general anaesthesia: 50, 000 IU up to 150, 000 IU against the three main causative agents: Cl. perfring-es, Cl. oedematiens, Cl. septicum. Serum is diluted with 300-400 ml of normal saline. Five prophylactic doses of serum are given intramuscularly. After the causative agent has been isolated, the appropriate serum is given. Prior to this, tests for the patient's tolerance of foreign protein: are done 0, 1 ml of serum are injected intradermally from a test ampoule in the concentration of 1: 100. If the size of the resulting blister exceeds 10 mm (with surrounding hyperaemia), the test is regarded as positive. If the test is negative, 0, 1 ml of serum are given again subcutaneosly (if in 30 minutes no reaction is seen, the preparation is injected either intramuscularly or intravenously). Detoxicating transfusion therapy is of vital importance - at least 4 l of fluid have to be given in 24 hours (polyion solutions; detoxicating solutions - haemodes (neocompensan); those that facilitate microcirculation - rheopolyglucin; glucose and protein solutions). The patient needs complete bed rest, balanced diet and supportive treatment. Antibacterial therapy involves the following drugs: 1. Antibiotics: • carbopenems; • vancomycin. 2. Chemical antiseptics: • metronidazole; • dioxydine (see «Biological antiseptics»). Hyperbaric oxygenation plays an important role in the complex therapeutic measures. This involves treatment in the chamber under the pressure of 2, 5-3 atmospheres. The method helps to reduce the extent of surgery required and to prevent a delay in the need for early amputation of the limb. Tetanus. Tetanus is a severe wound infection. The incubation period ranges from 4 to 14 days. Its early recognition is of critical importance. The classical triad of signs (trismus, facies tetanica and opisthotonos) can be observed in the late stages of the disease. It can be suspected when new local and general signs appear: shooting or twitching pain in the wound with irradiation along the nerve fibres, burning or tingling in the wound area, increased and localised sweating, and in some instances paraesthesia associated with muscular hypertonicity, and a change in the positioning of the limb. The early general signs include perspiration, weakness and difficulty in swallowing and require that the patient be immediately examined to exclude hyperreflexia and rigidity of muscles. During dressing, the wound has to be thoroughly examined, twitching of the muscles in the wound may be observed and when the wound is touched with forceps or a piece of gauze, a muscle twitch can occur. Remember to examine the muscle tonus, including that of the chewing muscles (rapping the chin with the patient's mouth open causes a sharp closure of the mouth as a result of spasm of the chewing muscles), occipital muscle rigidity (by way of bending the neck), muscles of the pharynx (by the act of swallowing). In advanced cases of tetanus, the patient will complain of fear and insomnia and will demonstrate agitation and wincing, fever and perspiration. The major signs of tetanus are muscular hypertonicity, rigidity, and tonic and clonic spasms. The «descending» form of tetanus starts with rigidity of the chewing and other facial muscles, while the 'ascending' one is characterised by initial rigidity of muscles around the wound. Spasms that are initially local develop with: trismus (lockjaw), dysphagia (spasm of the swallowing muscles), rigidity of the occipital muscles, spasm of the facial muscles (risus sardonicus) (fig. 80, colour inset). Progression of the disease leads to spread of the spasms over all other muscles of the trunk, spine, abdomen, with resultant opisthotonos - overextension of the body due to convulsive contraction of the long muscles of the back. Spasms need only minimum external stimuli to occur - light, noise or just a small push. The duration of convulsing ranges from a few seconds to a few minutes. The patient is conscious and has marked muscular pain. During general convulsive attacks, respiration arrest ensues, lasting the whole period of convulsions, and may even be fatal due to asphyxia. Convulsions usually develop parallel to general signs of infection: fever, tachycardia, and sweating. Treatment. The patient should be kept in a separate quiet and dark environment to be monitored for 24 hours; this helps notice the signs of impending seizures and provide the appropriate aid (control of spasms and respiratory arrest). Treatment must be started as early and involve anticonvulsive measures, airway management, detoxication, specific antibacterial and antitoxic therapy. In localised spasms sedative agents (diazepam, seduxen etc) are used, barbiturates, aminazin, droperidol etc. In severe generalised convulsions muscular relaxants together with barbiturates or diazepam may be used. Muscular relaxants have to be used with artificial lung respiration through tracheostomy for about 7-10 days, or in severe cases up to 30 days and longer, i.e. until spasms cease. Muscular relaxants and mechanical ventilation are indicated for short lasting initial stage of tetanus, fast progression of spasms, ineffectiveness of neuroplegic agents and barbiturates, in respiratory defect and aspiration pneumonia. Hyperbaric oxygenation is part of therapy. Specific therapy must be started as soon when the toxin is still circulating in the blood (after 2-3 days the toxin enters the neurons which renders antitoxins ineffective) The daily dose of the antitetanus serum is 100, 000-150, 000 IU, the total dose being up to 200, 000-300, 000 IU. Half of the daily dose is diluted with normal saline in the ratio of 1: 10 and infused slowly intravenously, while the rest is given intramuscularly (as a single dose). Antitetanus gamma globulin is administered intramuscularly (the total dose is as high as 20, 000-50, 000 IU, initially 10, 000 IU and then 5, 000 IU daily). In children, the total dose is 3, 000-6, 000 IU. Tetanus toxoids are given intramuscularly at 0, 5 ml three times each 5 days. Detoxication involves giving detoxicating solutions, those of electrolytes and glucose. Acidosis requires administration of solutions of sodium bicarbonate and trisamine. When the patient cannot eat, parenteral nutrition is provided (see Chapter IV) - 2, 000-2, 500 kcal/ day. Broad-spectrum antibiotics are also used for both prevention and therapy of suppurative complications (wound infections, pyogenic tracheobronchitis, pneumonia etc.). As an emergency measure, the wound (which is expected to be the entry site for the infection) should be inspected; the sutures are to be removed, the edges retracted and the wound washed with hydrogen peroxide. In extensive necrosis and foreign bodies in the wound secondary surgical debridement is done, collections of pus abscesses in the wound are incised and evacuated by draining. If at the time tetanus occurs the wound has already healed, the scar tissue should invariably be excised within the intact tissue, minute foreign bodies removed. Subsequently, the wound is left open without suturing. Specific tetanus prophylaxis is done both as a scheduled and emergency measure. To achieve active immunity to tetanus absorbed toxoids are given. Scheduled immunisation is indicated for the following subpopulations: the military, machine-operators, builders etc.: 0, 5 ml of toxoid are given twice once a month. Revaccination is done after one year - 0, 5 ml of toxoid are given, and repeated revaccination is done only after 5 years. Children below 12 years of age are vaccinated with the complex vaccine of DPT (diphtheria - pertussis - tetanus). The mode of emergent prophylaxis depends on the immune status of the patient (previously immunised vs. non-immunised). Those immunised are given 0, 5 ml of toxoid as a single dose. The non-immunised are given 1 ml of toxoid and 1, 500-3, 000 IU of antitetanus serum or 450-600 IU of antitetanus gamma globulin, 0, 5 ml of toxoid are given again after 1 month and to reliably provide immunity 0, 5 ml of the toxoid are given after 1 year. Burns. Burns are the damage to tissues caused by their exposure to thermal, chemical, electrical, or radiation energy. Classification A) Causes 1. Thermal. 2. Chemical. 3. Electrical. 4. Radiation. B) Depth of damage Degree 1 - damage to only the epidermis. Degree 2 - damage to the epithelium up to the basal layer. Degree 3 - damage to the dermis. 3a - epithelial necrosis with partial involvement of the basal layer; hair follicles, sweat and sebaceous glands are intact. 3b - complete necroses of the dermis, basal layer and part of the subcutaneous layer. Degree 4 - complete necrosis of the skin and underlying tissues. The severity of burns depends on the area and depth of damage. Assessment of the area of burns facilitates adequacy of the therapy. The methods currently used to calculate the area involved the are as follows: 1. The «rule of nine». According to this rule, the body surface regions are divided into areas that are multiples of 9%. Each of the following body regions comprises 9% of total surface burn area: head and neck - 9%, upper limb - 9%; anterior part of the trunk - 18%, the back - 18%, lower limb - 18% (thigh - 9%, leg and foot - 9%), the external genitals - 1%. 2. The «rule of palm». If the areas damaged are not so extensive and scattered on different parts of the body, the rule of palm is applied to determine the areas of deep burns in the basis of superficial ones. The size of an adult palm is about 1% of the body surface area. The «rule of nine» and the «rule of palm» (fig. 81) give an estimation of the area involved. More precise information can be obtained based on a direct measurement of the area (sterile transparent marked paper or film is placed on the burn surface, the contours of which are traced onto the paper; the sheet of paper is then cut along the contour line and placed on a marked net with known graduations (e.g. on a graph sheet). This method yields the absolute figures. Special tables with graduations made according to the body surface areas (cm2) can also be used (the face 500 cm2, or 3, 1%; scalp - the hairy part of the head - 480 cm2, or 3, 0%; chest and abdomen - 2990 cm2, or 18, 0%; the hand - 360 cm2, or 2, 25%; the back - 2560 cm2, or 16, 0%, etc.).
Fig. 81. Assessment of the burn area: the «rule of nines», the «rule of the palm». Assessment of the depth of burns. The classification of burns into superficial (degrees 1, 2, 3a) and deep (degrees 3b, 4) is primarily based on the skin's capability of regenerating through epithelization in superficial burns (fig. 82). Within the first few hours or even days following injury, it is difficult to assess the depth of burns. The evaluation of skin sensation is used. In superficial burns, pain sensation at the affected areas is intact or somewhat reduced, while in deep burns it is lost. In deep burns of a limb, unaffected areas below the affected ones become oedematous. The method of infrared thermography can also be used to determine the depth of burns (the areas with deep burns emit heat at a lesser degree than normal ones). The depth of burns can be established on days 7-14 following the injury. Evaluation of severity of burns. In adults, the rule of 100 can be used (age in years + general burns area in %: J60 - good prognosis; 61-80 - relatively good prognosis; 81 - 100 - doubtful prognosis; i101 - poor prognosis). Frank's index is known to be more specific and involves determination of both the area and depth of damage. It is based on the assumption that deep burns worsen the patient's status three times as much as superficial burns. Thus, if 1% of a superficial burn equals one point, a deep burn equals three points. The total sum is referred to as Frank's index. The prognosis is good if the index is below 30 sites, relatively good - 30-60 sites, doubtful - 61-90 and poor - above 90 sites. Burn disease. Burn disease is a constellation of clinical signs that result from superficial burns (degrees 2-3a) with a burn area of above 15% body surface and in deep burns of more than 10% body surface. The four periods of the disease are identified. 1. Burn shock. 2. Acute burn toxaemia. 3. Septicaemia. 4. Recovery. Burn shock. Being the major pathogenic mechanism of burn shock (erectile phase), loss of blood plasma results in local accumulation of vasoactive substances (e.g. histamine, serotonin) and an increase in blood viscosity, which consequently impairs microcirculation. The manifestations of burn shock, which may last 2-72 hours, depend on its duration and severity of circulatory defects (see «Shock»). Stabilisation of the latter may imply evolution to the further period of burn shock.
Fig. 82. Determination of burn depth. Acute burn toxaemia. Once toxic products enter the blood stream, circulating blood volume returns to the basal levels; on the other hand, this leads to severe intoxication. Burn toxaemia manifests by fever, pronounced tachycardia, dullness of heart sounds, anaemia, hypoand dysproteinaemia, abnormal hepatic and renal functions. Acute burn toxaemia continues for 7-8 days. Septicaemia. Septicaemia starts approximately on day 10 and is characterised by severe infection. Staphylococcus, Pseudomonas and Proteus spp and E. coli are common causative agents. In deep and extensive burns, suppuration of the burn wound may occur during toxaemia. During this period, patients with deep and extensive burns show signs of general deterioration, which in severe cases may present as weight loss, skin dryness and pallor, pronounced muscular atrophy, bed sores and contractures of joints. The separation of the necrotic eschar starts on days 7-10, the period being characterised by proliferation of microbes and development of varied septic conditions (e.g. pneumonia, pressure sores, and sepsis). Complete skin regeneration is indicative of the end of the septicaemic period. Recovery. Recovery is characterised by restoration of bodily functions, which have been affected previously, i.e. during the earlier three periods of the disease. As the functional organ changes (e.g. those of the heart, liver, kidneys) can persist for as long as 2-4 years after the trauma, the patients with a history of burn disease should be followed up regularly. First aid in burns should aim at terminating the burning process and cooling the burnt area. Cooling is achieved with cold water, ice packs, and snow and is to be continued for at least 10-15 minutes. After the pain has subsided, aseptic dressing should applied locally, and analgesics and non-steroidal inflammatory drugs, warm tea and mineral water are given to the patient. During this period, topical treatment (i.e. therapeutic bandages) should be avoided. Apart from analgesics, the patient is given neuroleptics and antihistamines prior to transportation that should be as long as an hour. If the patient is to be transported for a long distance, he/she has to be given intravenous infusion of plasma substitutes and solutions of electrolytes, oxygen therapy and general anaesthesia (nitrous oxide), large amounts of alkaline drinks and cardiovascular agents. Local treatment. The two topical (closed and open) methods are used for burns. First, primary wound toileting is done. The skin around the burnt areas is cleansed with swabs soaked in 0, 25% ammonium, 3-4% boric acid, benzene or warm soapy water, with subsequent application of alcohol. Pieces of clothing, foreign bodies, peeling epidermis are removed from the wound; large blisters are opened to drain their contents, minor ones being left alone. Fibrin deposits are usually left intact since it is under these where regeneration takes place. Excessively dirty burnt areas are cleansed with 3% hydrogen peroxide. Sterile gauze or tissues are used to dry the burnt surface. As a rule, the primary wound toileting is done after 1-2 ml of promedol or omnopon have been injected subcutaneously. The closed method (bandaging or covering with dressing material) is the most commonly used and has a number of advantages as follows: • isolation of the wound; • provision of optimum conditions for the application of topical agents; • the possibility of active movement of patients with extensive burns during transportation. Its pitfalls are the following: • labour intensiveness; • the expenditure of large amounts of dressing material; • painful change of dressing. The open method is void of these disadvantages. In addition, it promotes formation of the thick eschar on the burnt surface, which is aided by free flow of air over the area, ultraviolet rays or the use of agents that dry it and coagulate protein. It is difficult, however, to implement this method when dealing with patients with deep and wide areas of burns as it requires the use of special equipment (e.g. chambers, cage with electric lamps). Moreover, there is always a high risk of wound infection (e.g. nosocomial). When treated by the open method, superficial (degrees 2-3a) burns tend to spontaneously heal. The open method is indicated for facial, genital or perineal burns. The open method requires the use of ointments containing antibiotics (5 and 10% synthomycin emulsions) and antiseptics (0, 5% furacilin, 10% sulphacyl) three to four times a day. Suppurated wounds should be dressed. If granulation is found in the areas of deep burns treated with the open method, the closed method should be added. Each of these methods has its specific indications. At the same time, they can be combined, whenever necessary. Mafenid (5% aqueous solution or 10% ointment) is successfully used, especially when the microorganisms in the wound are resistant to other antibiotics. Silver-containing sulphonamides on hydrophilic base (ointment Sulfaraginum) are also widely used. These possess potent antibacterial properties and thus promote epithelization. In degree 2, burns it takes 7-12 days for the epithelium to form, while in 3a degree 3 to 4 weeks. In deep burns, eschar, either as wet or dry necrosis, forms for 3-7 days. In the former variant a spread of necrosis, severe suppuration with intoxication may commonly be found. The separation of dry eschar starts on days 7 to 10 and leads to formation of granulation mounds (spots), which completes by weeks 4 to 5. The eschar is step-wise separated from the underlying tissues and removed. In deep burns, the primary task within the first 7 to 10 days is to promote dry eschar formation by means of special lamps, ultrasound or treatment with 1-5% solutions of potassium permanganate. To fasten the separation of eschar, chemical necrectomy, proteolytic enzymes, 40-50% salicylic and benzoic acids are used. Surgical treatment involves several operations: early necrectomy, autodermaplasty, limb amputation and reconstructive operations. Circular burns of chest and limbs have to be treated by necrectomy. The operation helps reduce the pressure exerted on the underlying tissues. If possible, necrectomy should be performed in the first three days after trauma when shock has resolved. Indications for early necrectomy are as follows: 1. Deep burns involving 10-20% of the body surface, especially if simultaneous autodermaplasty may be possible to perform. 2. Burns involving fingers; in such cases it is necessary to prevent excessive scar (webbed fingers) that can affect digital functions. 3. In elderly burn patients, to prevent wound infection and to facilitate early mobilisation. Extensive necrectomy is to be done within the first seven days since at a later period the risk of septicaemia is rather high. Necrectomy performed at a time should by no means exceed 25-35% of the body surface area. Autodermaplasty is the only method applied for deep burns (degrees 3b and 4). For this operation split thickness skin flaps (dermatome plastic), full thickness flaps on vascular peduncles, as well as migrating (Filatov's) stalks are used. The skin graft (0, 2-0, 4 mm thick) is harvested from the intact skin, preferably taken from symmetrical areas with a dermatome. The operation can be performed either under local or general anaesthesia. To cover the burnt surface in deep burns cultured autofibroblasts or foetal fibroblasts can be used. This stimulates skin regeneration, which is especially effective if the skin growth layers have not been destroyed (degree 3b). The transplantation of the cultured fibroblasts is done in combination with that of split thickness net skin flaps. Principles of treatment and resuscitation. Resuscitation of the patient in the state of shock should be started at the stage of first aid and continued in hospital. Before admittance to hospital. 1. Give rest and apply dressing to the wound. 2. Give analgesics and antihistamines; during transportation in case of extensive burns - give phentanyl and droperidol, inhalation of nitrous oxyde in combination with oxygen. 3. Keep the patient (warm drinks, hot water bottles). 4. Compensate for plasma loss by giving alkaline solutions and parenteral infusion of fluids. When hospitalised, the patient is admitted into the antishock ward. The major task is to restore circulation and replace circulating blood volume by means of the following measures. — Administration of analgesics (fentanyl + droperidol), antihistamines. — Improving cardiac function by giving digitalis derivatives. — Improving microcirculation with euphyllin, intravenous droperidol and 0, 25% novocain). — Injection of hydrocortisone (125-250 mg) or prednisolone (60-90 mg) after circulating blood volume has been restored. — Oxygen therapy. — Restoration of renal function (mannitol, lasix in mild cases, intravenous infusion of 20% sorbitol solution in severe cases). — Early administration of bacteriophages, staphylococcal toxoid. — Transfusion of plasma solutions (native and dry plasma, albumin, protein, fibrin), whole blood, solutions that improve circulation, detoxication solutions, saline solutions (10% glucose, acesol, disol, trisol, lactosol). Burns involving above 10% of the body surface can lead to burn shock. Before burn shock develops, it is necessary to take preventive measures and give therapy (analgesia, replacement of plasma loss etc). It has to be taken into consideration that most plasma is usually lost within the first 8 to 12 hours and continues for about 2 days. In extensive burns, plasma loss can reach at least 6-8 l/day, the daily loss of protein being at least 70-80 g. There are several methods to calculate the fluid requirement, the principles of which can be as follows: 1. The volume of fluid given should not exceed 10% of the patient's body weight. 2. Within the first 8 hours after injury 1/2 or 2/3 of the daily amount of fluid required should be given. 3. On days 2 and 3, the amount of fluid given should not exceed 5% of the body weight. Of practical importance is the Brock's formula: [2 ml × body weight × the surface area burnt (unless the burn is of degree 1) + 2000 ml of 5% glucose solution. The effectiveness of treatment is assessed based on clinical features, haemoglobin and haematocrit values; of great importance are the serial central venous pressure values and those of hourly diuresis. Chemical burns. These are caused by concentrated solutions of acids and alkali (base), which leads to necrosis of the skin and mucosal membranes that may extend to deeper lays. Acids cause dry, or coagulation, necrosis, while alkali cause wet, or colliquative, necrosis. The common culprits are sulphuric, hydrochloric acid, and sodium hydroxide. Chemical burns are most commonly localised. Examination of the patient reveals burnt areas with clear borders. Strips of bands can be seen leading from the damaged areas, which form as a result of the trickling of the acid or base, or separate areas of necrotic spots are encountered when the chemical substance was sprinkled. Acids cause tissue dehydration, eschars form that are located deeper than the intact skin. When the burn is caused by sulphuric acid, the eschar formed is grey, dark brown or black, nitric acid - yellow, hydrochloric - grey yellow, acetic - greenish. Wet necrosis caused by alkali burns appears as a thick jelly mass of grey colour. The necrotic skin is on the same level with the intact skin or occasionally a bit swollen up. Chemical burns of the first and second degrees are considered superficial, third and fourth degree burns are regarded as deep burns. In first degree burns patients complain of pains, and burning sensation. Examination of the burnt area reveals an outlined area of hyperaemia with minimal swelling of the skin, which is more pronounced in alkaline burns. All types of sensory functions are intact, pain sensation is exaggerated. In second-degree burns dry (in acid burns) or jelly-like/soapy (in alkaline burns) superficial skin eschars are found. The eschar is very thin and easily creased. In deep (third and fourth degree) chemical burns, thick firm skin eschar is found, which cannot be creased. The eschar is immobile and appears as wet necrosis in alkaline burns and dry necrosis in acid burns. All types of sensation are lost. It is not possible to differentiate between third and fourth degree chemical burn at the first examination. In third degree of burns, all skin layers are necrotised, in the fourth degree, necrosis develops as deep as to the bone. It is only at the third - fourth week after injury when the eschar begins to separate and the depth of damage can be established: if only necrotised skin peels off then it is a third degree burn, in case deeper lying tissues separate, it is a fourth degree burn. First aid for chemical burns involves the removal of the chemical agent from the skin as early as possible (the first few seconds or minutes). It is more effective to wash the area under running tap water for 10-15 min, and if the washing was started late then it should be continued for 30-40 min; in fluoric acid burns washing is continued for 2-3 hours. Washing of the burnt surface should be continued until the smell of the chemical disappears or until the colour of the litmus paper placed on the area has changed. In burns caused by lime, washing is not allowed because the resulting chemical reaction produces more heat to lead to thermal burns in addition. When slaking lime pours on the skin, it has to be removed mechanically. After the chemical agent has been removed from the skin sterile dressing is applied and the patient is transported to the hospital. Electric burns. High-voltage electric current can cause electric burns at the entry and exit sites of the current. These kinds of burns are always deep, and here the underlying tissues are damaged than the skin itself. All the tissues on the way of the current get necrotic, the major vessels get thrombosed in addition. In view of these the extent of burn is not established by the skin damage, which is limited to about 2-3 cm in diameter, but by the damage caused to the deep lying tissues that come into contact with the current. When major vessels are damaged there can be tissue necrosis, gangrene of an organ e.g. a limb. On the sites of entry and exit of the current «current signs» form - burn wounds. The type of «sign» differs: circular, oval, with normally a diameter of 2-3 cm with the centre drawn in; in lightning treelike type. «Current signs» consist of grey or dark brown coloured eschars with depressed centres and oedema of the adjacent tissue. Skin sensitivity is decreased. The «figures» of lightning consist of dark greyish brown tree like forms. First aid to the person with electric shock should primarily be aimed at removing the patient from the current and starting resuscitation measures, if necessary (see Chapter X), and the places of burns should be covered with sterile dressing. When rescuing the patient from the current, it has to be remembered that touching the patient's body can also lead to injury of the one trying to help. Putting off the electricity connection to the source or cutting off the wire using a wooden handled axe or instrument with dry wood handle can rescue the patient. The wire is then pushed away with a stick, or board and the injured is pulled away to the side by his/her clothing. After the cardiac and respiration functions have been restored, dry sterile dressing is applied to the burnt areas. All persons after rescue from an electric shock must be sent to the hospital. In thermal burns as a result of breathing in hot air or gaseous substances or smoke there can be burns to the respiratory tract. Breaking of the voice (hoarseness), hyperaemia of the mucus layers of the throat and mouth with white patches and traces of soot are all signs of burns to the respiratory tract. Frost bite (freezing). This involves local damage to the skin and deep lying tissues because of extreme cold resulting to blood circulatory failures. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 71; Нарушение авторского права страницы