|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Mechanical and physical antisepsis
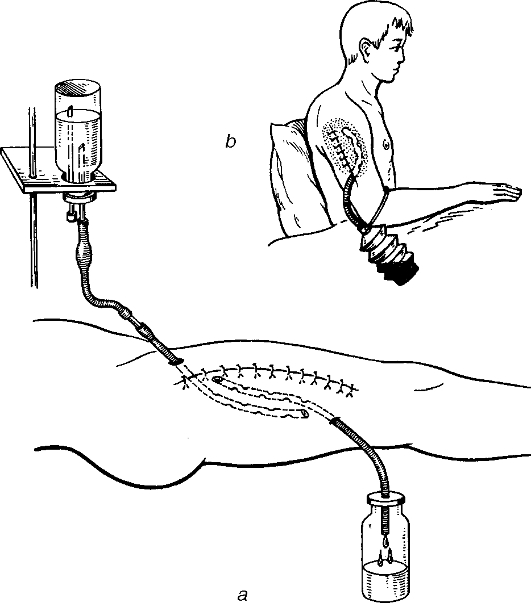
Mechanical antisepsis is based on surgical debridement of wounds. This is performed in the surgical theatre and involves excision of the edges, walls and the floor of wounds to remove the non-viable tissue and microorganisms within the wound. It is the major method to treat accidental, infected wounds (see «Wounds»). Physical antisepsis starts from the law of capillarity, hygroscopicity, diffusion, osmosis, siphoning, ultrasound and laser effects. These are the principles used: • to enhance drainage from wounds and pus from abscesses and empyemas, • to facilitate flow to the outside (into a dressing or a special container with antiseptic solution). For the treatment of wounds, a gauze pack is used as the drain. Packs of different sizes are made of gauze strips and packed loosely into the wound; owing to their hygroscopic qualities the swab absorbs blood, exudates and pus. Its draining capacity lasts as long as 8 hours. Following this, it turns into a «plug» that blocks the wound and inhibits the flow of exudates outside. To increase the drainage capacity of dressing, the pack is soaked in hypertonic solution (5-10% sodium chloride). This yields a higher osmotic pressure and therefore enhances the flow of liquids from the wound into the dressing. Apart from the ordinary pack, Mikulin's swab can also be used. A big gauze napkin with a thread sewn into the centre is packed into the wound. The napkin is placed on the floor and walls of the wound to form a packet, which is filled with gauze swabs or packs. When the swabs get soaked with secretions, the former need to be replaced with new ones, the big gauze napkin being left alone. The packs are changed several times until they appear to contain no pus. Following this the main gauze napkin is removed by drawing the thread. Wounds can also be drained by using plastic, vinylchloride or other tubes of different diameters, which are placed in the wounds, abscess cavity, joints (in purulent arthritis), pleura (in purulent pleuritis), abdominal cavity (in purulent peritonitis). The pus, products of tissue decay, and microorganisms are discharged through one or several drains into the dressing. The drain can be connected by a tube to a container with an antiseptic; thus the secretions empty into the container which prevents pollution of the dressing. Chemical antiseptics, antibiotics, proteolytic enzymes can be inserted through the drainage into the wound or cavity. To provide a more effective washout of wounds and purulent cavities, apart from the drainage tube, another tube can be placed, through which antibacterial agents can be given and pus, products of tissue decay, blood and fibrin are discharged (fig. 5). Hence a combination of physical and chemical antisepsis results in continuous irrigation drainage. This method is also used in purulent pleuritis and peritonitis. To enhance its efficacy, proteolytic enzymes are used as the washing solution, which promotes lysis of non-viable tissues, pus and fibrin (enzymatic irrigation dialysis method).
Fig. 5. Through (a) and suction (b) wound drainage. If the draining cavity is sealed (sutured wound, pleural empyema, purulent arthritis, abscess), active aspiration, or vacuum drainage, can be used. Negative pressure in the system can be reached with Janet's syringe which is used to evacuate air from a sealed bottle connected to a drainage tube, or with the aid of flowing-water suction or a three-bottle system. This is known to be the most effective way of drainage. It also helps reduce the size of the wound cavity and cause fast obliteration and removal of infection, and facilitates expansion of the lung collapsed as a result of the pressure of exudates in pleural empyema. Chemical antisepsis Synthetic antibacterial agents are used to combat bacterial infection in the wound or inflammatory foci. These are both effective for therapy and prophylaxis and help achieve antibacterial effect inside the human body. • Derivatives of nitrofuran. These agents are effective against purulent cocci. — Furacilin Aqueous solution (1: 5, 000) is used for washing out purulent wounds during dressing, washing out abscess cavities and empyemas through the drainage tube (e.g. in purulent pleurisy and purulent fistula of osteomyelitis). — Soluble Furagin (Furagin K- or Furagin-potassium, Solafur) The indications of its 0, 1% solution are similar to those of furacilin. It can also be given intravenously in a dose of 300 ml. Orally, furazolidon is taken as 50 mg tablets. Derivatives of nitrofuran may also be ingredients of the membranous compound lifusol manufactured as an aerosol and used to treat superficial wounds and burns. It forms a defensive membrane that causes antimicrobial effect on the wound's surface. Effect of this membrane lasts for 5-7 days. • Acid group For washing wounds, purulent cavities and purulent fistulae, 2-3% aqueous solution of boric acid is used. • Oxidants This group involves hydrogen peroxide and potassium permanganate, which, if combined with organic compounds, discharge atoms of oxygen, which cause antimicrobial effect. — Hydrogen peroxide is used for cleaning infected wounds during dressing, purulent fistulae, empyemas and abscesses in the form of 3% aqueous solutions. The thick foam that is formed during the washing facilitates evacuation of pus, fibrin and necrotic tissues. It can also neutralise the offensive odour of the wound. — Potassium permanganate is indicated for purulent wounds (0, 1-0, 5% solution), washing cavities (0, 05-0, 1% solution) and burns (2-5% solutions). • Dyes — Brilliant green is used as a 1-2% alcohol solution for superficial wounds, abrasions and suppurative skin infections. — Methylene blue is used for superficial wounds and abrasions (3% alcohol solution), burns (1-2% alcohol solution) and for washing purulent cavities (0, 02% aqueous solution). • Detergents — Chlorhexidine. The main aqueous solution contains 20% of chlorhexidine bigluconate. For cleaning wounds, a 1: 400 solution is available, for washing infected bodily cavities a 1: 1, 000 may be used. 1 ml of 20% aqueous solution of chlorhexidine bigluconate is diluted in 400-1, 000 ml of distilled water. The solution is sterilised in an autoclave at a temperature of 115 °C for 30 minutes. • 5-Nitro-imidazole derivatives — Metronidazole; trade names - flagyl, trichopol, clion. It is effective against non-clostridial anaerobes and can be given intravenously (0, 5 g in 100 ml of solvent). Dioxydin. This is a derivative of oxychinolin. 0, 1-1% aqueous solutions are indicated for purulent wounds, for washing the urinary bladder, empyema or abscess cavities, and purulent fistulae. It is available as 10 ml ampoules with 1% solutions of the drug. In severe purulent infections (sepsis, purulent peritonitis), it can be infused intravenously as much as 60-90 ml 2-3 times a day (30 ml of the solution diluted in 500 ml of 5% glucose solution). It should be avoided in patients with impaired renal function. • Heavy metal salts — Silver nitrate is used as 0, 1-0, 2% solutions for washing wounds and purulent cavities. Sulphonamides (streptocide, ethazol, sulfacyl) Derivatives of sulfacyl with prolonged activity (sulfadimethoxin, sulfalen, sulfapiridazin) are available as tablets. Topical chemotherapy involves: a) application of antiseptics to dressing materials for wounds and burns; these may be applied in the form of solutions used to wash the wounds during dressing, soaking the dressing packs as well as in the form of creams and powders; b) application of antibacterial solutions directly into the wound, closure of the cavity with subsequent aspiration through a drain - washing, leaking drainage (i.e. a combination of physical and chemical types of antisepsis). Examples of combined use of physical and chemical antisepsis are peritoneal dialysis for purulent peritonitis, leaking drainage of pleural cavity in purulent pleuritis; c) infiltration of foci of inflammation with antibacterial solutions to combat local infection (antibiotics are often used for such purposes). Systemic chemotherapy includes: a) oral use of antibacterial agents: tablets of Furagin, Solafur, long-acting and very longacting sulfonamides (sulfadimethoxin, sulfalen) which act topically on gastrointestinal microorganisms; this is part of preoperative workup for patients with impending intestinal surgery. Absorbed into the blood stream, these drugs also act on the body systemically after they have been absorbed into the bloodstream; b) intravenous use of chemotherapeutic compounds: e.g. soluble furagin, dioxidin Biological antisepsis For treatment and prophylaxis of purulent infections biological compounds can also be used. Antibiotics are known to be of greatest importance as far as antibacterial therapy is concerned. Currently, the use of antibiotics has been facing a multitude of problems associated with changes in biology of target microorganisms, i.e. quite a number of drug-resistant strains have emerged. The main causative agents of purulent infections - staphylococci and gram-negative bacteria (e.g. E. coli, Proteus spp, Pseudomonas aeruginosa)have become highly resistant to antibiotics as a result of mutations caused by antibiotics. Among the causative agents of purulent infectious diseases, relative pathogenic microorganisms (non-obligatory pathogens) make up a separate group - non-sporiferous (nonclostridial) anaerobes and mainly Bacteroides, which have a natural resistance to most antibiotics. The major antibiotics used for treatment and prophylaxis of infections are as follows: • The penicillins One of the first antibiotics was a natural antibiotic benzylpenicillin still used nowadays in selected cases. The main advantage of bewzylpenicillin is low foxicity. Semisynthetic penicillins fall into the two groups: 1) stable penicillins (oxacillin, metycillin, dicloxacillin), which are active against gram-positive bacteria. They are indicated for staphylococcal infections of various localization (pneumonia, lung abscess, pleural empyema, osteomyelitis, abscess or phlegmon of soft tissues, wounds), 2) broad-spectrum semisynthetic penicillins (ampicillin; ampiox - a combination of ampicillin and oxacillin; carbenicillin). These are effective in burns, peritonitis, infected wounds caused by Pseudomonas and Proteus spp. • Cephalosporins Firstand second-generation cephalosporins include ceporin (cephaloridin), kefzol (cefazolin), cephalothin, and cephalexin; cephataxime, cefotaxim, ceftriaxon are third-generation cephalosporins, and cephpirom (Quiten) belongs to fourth-generation cephalosporins. • Aminoglycosides These include gentamicin, kanamycin, tobramycin and semisynthetic aminoglycoside (amikacin). • Tetracyclines These include tetracycline, oxytetracycline and semisynthetic tetracyclines (metacycline or rondomycin), doxycycline (vibramycin). • Macrolides These include erythromycin, oleandomycin, azithromycin. • Fluorquinolones (ofloxacin, pefloxacin, ciprofloxacin, lomefloxacin) are a group of antibacterial agents whose bactericidal effect is based on the block of DNA gyrase of the susceptible bacteria. Their broad spectrum of activity covers numerous gram-negative and gram-positive microorganisms (e.g. E. coli, Enterobacteriaceae, Klebsiella and Staphylococcus spp). Other groups of antibiotics used to combat purulent infections are lyncomycin, fusidin. Broad-spectrum antibiotics that act bactericidal on both gram-negative and -positive strains are semisynthetic penicillins, cephalosporins and aminoglicosides, semisynthetic tetracyclines, fluorquinolones (ofloxacin, ciprofloxacin, levofloxacin). carbopinems (imipenem, pleropenem, tienam (a combination of imipenem + sodium celastatin). Biologic antiseptic compounds include proteolytic enzymes. They can dissolve (lyse) necrotic tissues, fibrin, pus, prevent oedema and enhance the therapeutic effect of antibiotics. The currently used proteolytic enzymes of animal origin are trypsin, chymotypsin, chymopsin, ribonuclease; those of bacterial origin - terrilitin, streptokinase, collagenase, asperase, ribonuclease, iroxol; plant origin - papain, bromelain. Proteolytic enzymes can also be used topically for infected wounds or tropical ulcers. After cleaning the wound or ulcer with hydrogen peroxide or furacillin, a piece of gauze soaked with the solution of enzyme is applied on it; if the wound is highly purulent, the powder of the enzyme can be sprinkled on its surface. Some of the enzymes are available in the form of cream (iruxol, asperase), which are also applied to the wound or sore. These are used until the wound is clean of all the necrotic tissues and pus. Their doses may be different and are usually given in their instructions. Solutions of enzymes can be introduced into various cavities: the pleural cavity in purulent pleurisy, the joint cavity in purulent arthritis or in an abscess cavity. The drug is given through a drainage tube after puncturing the cavity; the contents being then aspirated. In lung abscess that may not be drained through the bronchus, a special method (via a puncture of the chest wall) is used. In osteomyelitis the enzymes are given into the canal of the bone marrow or into the bone cavity by puncturing the bone with a needle or through a drainage tube placed during operation. In purulent fistulas the canals can be washed with the solutions of enzymes. In purulent lung infections proteolytic enzymes can be inhaled or they can be inserted into the bronchi or through a catheter or bronchoscope into the abscess cavity. In infectious infiltrations, enzymes (trypsin or chemotrypsin) can be given via electrophoresis. As anti-inflammatory agents proteolytic enzymes (trypsin, chemotrypsin) are given intramuscularly or intravenously in doses of 0, 07 mg/kg. Proteolytic enzymes dissolved in solutions of novocain (procaine) can be used to infiltrate tissues at the initial stages of inflammations or added to the solutions used for novocain blockage. For example, at the initial stages of mastitis retromammary blockage can be performed (see «Local anaesthesia»): 70-80 ml of 0, 25% novocain, 10 mg of chemotrypsin or trypsin and 500, 000 units of kanamycin are injected into the retromammary space. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 196; Нарушение авторского права страницы