|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Spinal and peridural anaesthesia
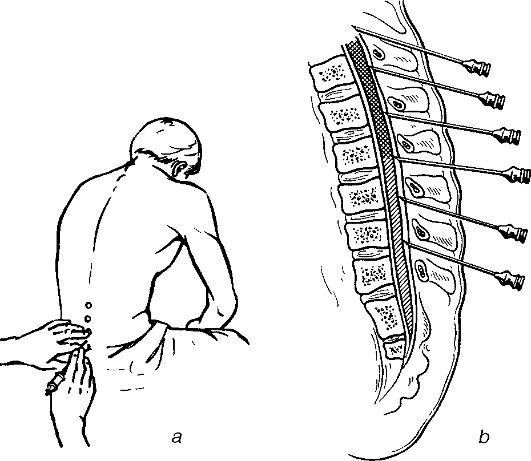
Spinal anaesthesia is a nerve block-type anaesthesia. It is done by injecting the anaesthetic into the subarachnoid space of the spinal cord and indicated for operations on the organs below the diaphragm (the stomach, intestine, liver and bile ducts, spleen, the pelvic organs) as well as the lower limbs. The anaesthetics block the posterior, or sensory, spinal roots, which leads to the loss of various sorts of sensation, and anterior, or motor, roots that causes muscular relaxation. Preganglionic sympathetic fibres that pass through the anterior roots are also blocked, which results in dilation of the local arterioles. When sympathetic fibres contributing to the coeliac nerves are blocked, the vascular dilation of abdominal and pelvic organs and the lower limbs can lead to the storing of blood into them and hence a fall of blood pressure. Special spinal needles with well-fixed mandrin, syringes with tenth-millilitre graduations are used. 5% novocain, 1% ultracain, 1% trimecain or 2% lidocain is used. 2 ml of 20% caffeine solution and 1 ml of 5% ephedrine solution are given to the patient 30 minutes prior to the operation. The patient is set on a table, his/her feet put on a step, the knees raised a little and the spine in maximally flexed. The nurse standing in front of the patient presses down on his/her shoulders and helps to keep him/her in the required posture. If the puncture is to be done with the patient lying, he/she is put on a table lying on the side, the back at the edge of the table with the knees raised to the stomach and the chin lowered to touch the chest, the spine being maximally flexed. An assistant stands in front and with his/her one hand on the patient's neck and another on the hip fixes him /her as if trying to fold out his/her spine where the puncture is to be done. The lumbar puncture is usually performed between L3 and L4 or L2 and L3 vertebrae processes. Lumber spine L4 is used as the hallmark of the line joining the superior posterior spines of the iliac bones (fig. 15). The operative field is cleansed with ether and alcohol. The skin of the injection site is infiltrated with 0, 25% novocain. The needle is placed in the midline in between the bone processes tilted a little (5-10°) downwards. When the needle passes through the intervertebral and yellow ligaments, some resistance, which vanishes after passing through, is felt. Some more resistance is encountered at the point of entry through the spinal dura matter, after this the guidance of the needle is stopped, the mandrin removed and the needle rotationally pushed forward for 2-3 more mm piercing the internal layer of the dura matter. The appearance of colourless fluid suggests successful puncture. If there is no or just a little fluid, the needle is rotated around its axis and advanced for about 1-2 mm. If there is still no fluid or blood appears, the needle is withdrawn and the process repeated through a different intervertebral space.
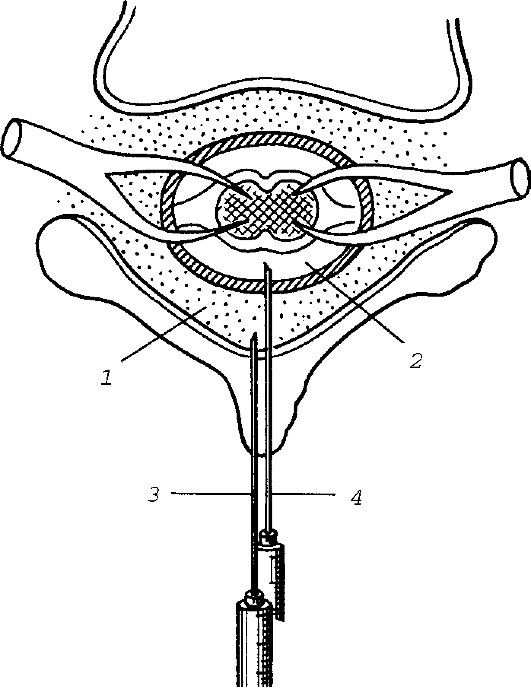
Fig. 15. Lumbar puncture. a - choosing the optimum puncture site; b - directing the needle depending on the vertebral spinal slope. After successful puncture, 2-3 ml of cerebro-spinal fluid are drawn into the syringe, mixed with 2 ml of 2% lidocaine or 1 ml of 5% novocain and then injected into the cerebrospinal canal. The patient is immediately placed on the operating table with the head end of the table raised. With this the anaesthetic is prevented from spreading to upper areas of the spinal cord and to the midbrain. Contraindications for spinal anaesthesia: • traumatic shock; • severe intoxication as a result of peritonitis; • concurrent hypotension; • myocarditis; • cutaneous infections on the spine; • vertebral column deformity. Complications A serious complication of spinal anaesthesia is a fall in blood pressure, which results from block of the sympathetic nerve fibres. This type of complication often occurs when anaesthesia is performed at the level of the lower thoracic or upper lumbar spines; the complication is very rare when the puncture is performed at the lower lumbar spines. To prevent hypotension, vasoconstrictors may be given before or during the procedure, transfusion therapy may also be of use. To centralise blood circulation, the lower limbs are bandaged and raised. When the anaesthetic spreads upwards along the subarachnoid space, it can block the innervation to the intercostal muscles that control breathing hence affect it or even cause respiratory arrest. Oxygen therapy is used to treat pulmonary insufficiency, and if respiratory arrest is obvious, mechanical ventilation is required. Headaches, lower limb paresis, suppurative meningitis can occur following spinal anaesthesia. Because of its serious complications spinal anaesthesia is only rarely used. Recently, peridural anaesthesia has become widely used. Peridural anaesthesia is a type of nerve block anaesthesia. The anaesthetic, given into the peridural space between the dura matter and the periosteum of the vertebrae, results in the block of the spinal nerve roots (fig. 16). This method of anaesthesia imparts all the advantages of spinal anaesthesia and is void of all its disadvantages.
Fig. 16. Epiand subdural puncture. 1 - epidural space; 2 - subdural space; 3 - the needle at the epidural space; 4 - the needle at the subdural space. Technically, the puncture of the peridural space is similar to that of subdural space. The puncture can be performed at any level of the vertebral column. It is noteworthy that the dura matter can easily be punctured, which will facilitate entering the drug into the subarachnoid space with resultant serious complications. The puncture is done with a needle connected to a syringe that contains normal saline solution. Resistance accompanies movement of the needle on pushing on the syringe until is passes through the intervertebral ligament and enters the peridural space, when no resistance is endured and the liquid is easily injected. Further evidence of the needle being in the correct space is that when the needle is connected to a water manometer, cerebrospinal fluid should not gush out, there should be a negative pressure reading on the manometer. Anaesthetic can be given with a needle or through a catheter which is introduced through the needle and left for a long period. To lengthen anaesthesia the drug can be given through the catheter in fractions. Up to 40 ml (fractionaly) of 1-2% lidocain or trimecain are introduced into the peridural space. Peridural anaesthesia is used during trauma and orthopedic surgeries on the lower limbs, abdominal and pelvic operations. This kind of anaesthesia is used for old and elderly patients, those with serious cardiovascular and respiratory diseases, patients with metabolic disorders (obesity, diabetes mellitus). Contraindications for peridural anaesthesia are similar to those for spinal anaesthesia. Complications are very rare. Hypotension and respiratory problems, nausea, vomiting and seizures can occur. Anaesthesia may not be achieved in 5-10% of cases, which is accounted for by the presence of possible adhesions in the peridural space that prevent entry and spread of the anaesthetic drug. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 96; Нарушение авторского права страницы