|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Which method is that of mechanical antisepsis?
A. Through drainage. B. Vacuum drainage with electric motor causing negative pressure in a closed drainage system. C. Primary surgical debridement. D. Ultrasonic cavitation of wounds. E. Through drainage with proteolytic enzymes. Choose the correct answer. 2. Methods of physical antisepsis are as follows: 1. Drainage of subcutaneous connective tissue. 2. Irrigation of the wound with chlorhexidine solution. 3. Necrectomy. 4. Ultrasonic cavitation. 5. Immunotherapy. Choose the right combination of answers: A. 1, 2. B. 2, 3. C. 1, 4. D. 2, 4. E. 3, 5. 3. Agents that work as biological antiseptics are as follows: 1. Vaccines and sera. 2. Sulphonamides. 3. Nitrofurantoins. 4. Antibiotics. 5. Proteolytic enzymes. Choose the right combination of answers: A. 1, 2, 3. B. 2, 3, 4. C. 1, 4, 5. D. 1, 2, 5. E. 1, 3, 5. 4. The methods of physical antisepsis are as follows: 1. Ultrasonic cavitation of wounds. 2. Antibiotic and novocain block of the suppurative focus. 3. Through drainage. 4. Cauterizing of superficial wounds with silver nitrate. 5. Vacuum drainage of wounds. Choose the right combination of answers: A. 1, 4, 5. B. 1, 2, 3. C. 3, 4, 5. D. 1, 3, 4. E. 1, 3, 5. 5. Oxidizing antiseptics are as follows: A. Dichloride of mercury. B. Potassium permanganate. C. Carbolic acid. D. Chloramine. E. Silver nitrate. Choose the correct answer. 6. Haloid antiseptics are as follows: A. Potassium permanganate. B. Dichloride of mercury. C. Carbolic acid. D. Chloramine. E. Silver nitrate. Choose the correct answer. 7. The following antibiotics exert toxic effect on the auditory nerve: A. Penicillins. B. Aminoglycosides. C. Tetracyclines. D. Cephalosporines. E. Macrolides. Choose the correct answer. 8. The complications of antibacterial therapy are as follows: 1. Intestinal dysbiosis. 2. Hypertension. 3. Deafness. 4. Allergic reactions. 5. Tachycardia. Choose the right combination of answers. A. 1, 2, 3. B. 1, 3, 4. C. 2, 3, 4. D. 3, 4, 5. E. 2, 4, 5. 9. Errors of antibacterial therapy are as follows: A. Combination of antibiotics with nystatin. B. Combination of antibiotics of the same mechanism of action. C. Combination of antibiotics and proteolytic enzymes. D. Combination of several routes of antibiotic administration. Choose the correct answer. 10. The mechanisms of action of proteolytic enzymes are as follows: 1. Necrotic tissue lysis. 2. Hypercoagulation. 3. Fibrinolysis. 4. Enhancement of antibiotic activity. 5. Oedema counteraction. Choose the right combination of answers: A. 1, 2, 3, 4. B. 1, 3, 4, 5. C. 1, 2, 4, 5. D. 1, 2, 3, 5. E. 2, 3, 4, 5. Which agents promote non-specific immune response 1. Anti gas gangrene serum. 2. Anti staphylococcal anatoxin. 3. Prodiogiosane. 4. Levamisole. 5. Antitetanic serum. 6. T-Activine. Choose the right combination of answers: A. 1, 3, 5. B. 2, 4, 6. C. 3, 4, 6. D. 3, 4, 5. E. 4, 5, 6. 12. Proteolytic enzymes of animal origin are as follows: 1. Papain. 2. Trypsin. 3. Chymotrypsin. 4. Streptokinase. 5. Terrilytin. Choose the right combination of answers: A. 1, 2, 3. B. 1, 5. C. 2, 3. D. 2, 3, 4. E. 1, 4. 13. Active immunization can be performed using the following preparations: 1. Anti staphylococcal anatoxin. 2. Anti staphylococcal globulin g. 3. Bacteriophage. 4. Levamisole. Choose the right combination of answers: A. 1, 3, 4. B. 1, 2, 4. C. 1, 2, 3. D. 2, 3. E. 1. 14. The preparations which increase patients' non-specific immune protection: 1. Prodiogiosane. 2. Anti staphylococci anatoxin. 3. Lysozyme. 4. Bacteriophage. 5. Levamisole. Choose the right combination of answers: A. 1, 2, 3. B. 2, 3, 4. C. 1, 3, 4. D. 1, 3, 5. E. 1, 4, 5. 15. The high-power laser beams exert the following actions: 1. A change in biochemical tissue reactions. 2. An increase in tissue temperature. 3. A destruction of microorganisms. 4. An abrupt increase in intracellular and interstitial pressure. 5. An acceleration in immature cell proliferation. Choose the right combination of answers: A. 1, 3. B. 1, 5. C. 1, 3, 4. D. 3, 4, 5. E. 1, 2, 3, 4. Chapter II. ANAESTHESIA
Local anaesthesia is a reversible loss of sensation in some part of the body induced by a local anaesthetic agent. The advantages of local anaesthesia involve the following: • prolonged preoperative preparation is unnecessary; • it can be used when general anaesthesia (narcosis) is unavailable; • there is no need for postoperative observation of the patient, as distinct from narcosis. Outpatient surgeries are often done under local anaesthetics. Similarly, when intubation narcosis is risky, the patient can be operated on under local anaesthetics. Elderly patients, particularly debilitated ones, as well as those with cardiovascular disease are at increased risk, as far as postoperative mortality rate is concerned. In such cases anaesthesia may outweigh the risk of the operation itself. Contraindications for local anaesthetics are as follows: 1. The patient's intolerance of local anaesthetics drug (e.g. due to allergies). 2. The patient's age below 10 years. 3. Concurrent psychiatric disease. 4. Scarring or pronounced inflammation of the tissues within the operative field, which may interfere with the infiltration of the anaesthetic. 5. Intractable internal bleeding which requires urgent operation. 6. Thoracic surgery. Potentiated local anaesthesia can be achieved by combining anaesthetics with neuroleptic drugs (e.g. droperidol) and general analgesics (e.g. phentanyl). In combined anaesthesia, which includes local anaesthesia and neuroleptic analgesia, local anaesthetic effect is enhanced by the positive action of the neuroleptic and the patient's psychic status. Neuroleptic analgesia and general anaesthesia are used to potentiate different kinds of local anaesthesia (infiltration, trunk block, spinal, epidural). With the aid of neuroleptic analgesia and general anaesthesia the dosage and therefore the toxic effect of local as well as narcotic agents can be reduced. Complications of local anaesthesia are related to allergic reactions of the anaesthetic drug or its overdose or that of epinephrine. Allergy to a local anaesthetic drug is manifested by skin rash, itching, Quincke's oedema, laryngoand bronchospasm. Antihistamines, glucocorticoids and spasmolytics are used to counteract the allergic reactions. Overdose of local anaesthetic substances occurs if large amounts of the drug are injected. Symptoms of overdose are anxiety, skin hyperaemic, fast pulse, hypertension, twitching or convulsions. In serious cases of intoxication the patient can develop collapse, respiratory or cardiac arrest or even coma. Mild cases of overdose can be managed with barbiturates, narcotic agents and oxygen therapy. Serious cases may require inotropic and vasopressor agents are given, and transfusion therapy with car-diopulmonary resuscitation may be necessary. Prevention of the complications includes a thorough interviewing the patient as to drug allergies and meticulous following the protocols of anaesthesia. The main local anaesthetics and their properties are presented in tab. 1. Table 1. Local anaesthetic agents
Tab. 1. Contd.
During preoperative workup the patient is prepared psychologically for local anaesthesia. This derives from the fact that he/she will be conscious during the operation and his/her tactile sensation, as distinct from pain, will be intact. Before the operation preanaesthetic medication (injection of promedol, atropine, droperidol) is given to each patient. It is noteworthy that patients who develop minute psychiatric problems are put on sedatives and anti-anxiety agents for several days preoperatively. INFILTRATION ANAESTHESIA This type of anaesthesia is named after a famous Russian surgeon Alexander Vishnevsky. This way of anaesthesia combines the positive aspects of both infiltration and block anaesthesia. Anatomically, the method is based on the features of fascicular structures. The anaesthetic that is given under pressure into fascicular compartments spreads to engulf and penetrate the nerve and nerve ending. Tense infiltrates of novocain trickle along the fascial covering and converge with each other. Alexander Vishnevsky named his method the tense-creeping infiltrate. It is the surgeon who is in charge of anaesthesia during the operation - he/she interchanges the injection and the scalpel during incision. Tissue infiltration should precede opening the skin or fascial covering. Tense infiltration of anaesthetic allows for hydrous dissection of the tissues, in the mist of the infiltration it is easier to identify blood vessels, nerves and thus prevent their damage and enhance ligation of vessels to arrest bleeding. For infiltration anaesthesia to achieve, 0, 25% novocain with epinephrine (0, 15 mg of epinephrine to 100 ml of novocain) is used. Fascial covering anaesthesia requires a large amount of anaesthetic (as much as 800-1, 000 ml), but because of the low concentration of anaesthetic and the fact that most of the solution pours away through the wound during operation, patients are unlikely to get intoxicated. Thyroid turgeny may save as an example of that type of anaesthesia. Two syringes (a 2- and 5- ml or 5- and 10- ml ones are normally used for the injections. To anaesthetise the skin a small needle is used intradermally to form «peau d'orange» along the intended incision line (fig. 6). Each further injection follows the previous one. Novocain is injected also into the subcutaneous fat through the infiltrated skin. Adequate infiltration is achieved when the whole area of incision becomes raised in the form of a fold. After incision of the skin, subcutaneous layer and subcutaneous muscle of the neck, the anaesthetic is injected through the midline, infiltrating the muscles, then under the muscles directing it upwards, downwards and to the sides.
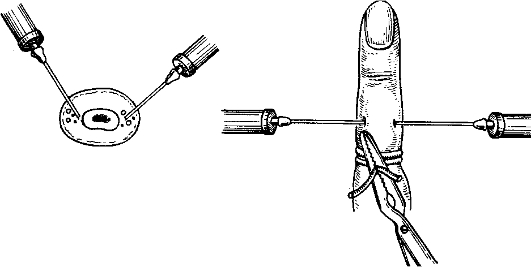
Fig. 6. Infiltration anaesthesia for thyroid surgery. a - anaesthetising the skin and subcutaneous tissue along the line of incision; b - injecting novocain beneath the cervical muscles; c - trickling infiltrate surrounding the thyroid gland. Novocain injected under the muscles spreads beneath the medial cervical fascia to surround the thyroid gland in the form of a case. After dividing the cervical muscles and delivering the thyroid gland into the incised wound additional infiltration of anaesthetic is given at the upper and lower poles of the gland as well as its posterior aspect. BLOCK ANAESTHESIA The following types of block anaesthesia are identified: • anaesthesia of the neural trunks; • anaesthesia of the neural plexuses; • anaesthesia of a group of the nerve ganglia (paravertebral anaesthesia); • spinal anaesthesia; • epidural anaesthesia. Block anaesthesia of the finger by Oberst-Luka-shevich. This method is used to operate on the fingers (for abscess, trauma or tumours). Two or three millilitres of 1-2% novocain are injected into the side of the phalanx as follows (the same amount of novocain is used to anaesthetise the other side of the finger): a plastic tourniquet is applied to the base of the finger, distal to which the skin is anaesthetised, followed by the subcutaneous and further to the bon injections (fig. 7). Novocain is thus injected directly onto the nerves of the finger, which pass along its lateral aspects.
Fig. 7. Conduction anaesthesia (Lukashevich and Oberst's method). INTERCOSTAL NERVE BLOCK This type of anaesthesia is used in rib fractures. A few centimetres away from the fracture site towards the spine, the skin is anaesthetised by intradermal injection of novocain, using a needle and syringe (fig. 8). Novocain is injected through the needle, slowly pusher in the perpendicular direction as long as it luts the fractures. Then the needle is pulled back for about 2-3 mm and is directed to the lower end of the rib along the lower surface and 3-5 ml of 1-2% of Novocain are injected. Passing onto the upper side of the same rib 2-3 ml of 1-2% novocain are injected after which the needle should be removed. In multiple rib fractures the procedure is repeated at the affected sides.
Fig. 8. Intercostal anaesthesia. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 241; Нарушение авторского права страницы