|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
STEPS OF CARDIOPULMONARY RESUSCITATION (CPR)
CPR comprises the four steps (ABCD): 1) A irway (removal of any loose obstruction in the respiratory tract); 2) B reathing (institution of artificial ventilation); 3) C irculation (closed chest massage); 4) D ifferential diagnosis, d rug therapy, d efibrillation. Lay persons are normally trained to perform the first two steps of CPR. Conversely, specific population categories (e.g. the military; police, especially those of the road traffic units; the fire service; water safety guards) and nurses should be able to provide the third step measures, namely closed heart massage. The first three steps can be taken outside hospital and not necessarily by people with some medical background. In contrast, step four of CPR is to be performed by urgent medicine specialists as well as staff of the intensive care unit. Step I (removal of any loose obstruction in the respiratory tract). Mucus, sputum, vomitus, blood or foreign bodies usually account for obstruction in the mouth and pharynx. It may also be accompanied by the tongue obstructing the entrance to the trachea due to mandibular muscle relaxation. The victim is placed supine on a hard surface, with the head turned aside, the 2nd finger crossed over the thumb of the right hand is used to open the mouth and a handkerchief or napkin wrapped around the 2nd and 3rd fingers of the left hand are used to clean the oral cavity (fig. 18). The head is now turned straight and maximally tilted backwards. In doing this one hand is placed behind the neck, the other on the forehead fixing the head in the tilted position. In bending the head backwards the lower jaw is pushed up together with the root of the tongue, which restores the free passage of the airway (fig. 19).
Fig. 18. Cleansing the oral cavity of mucus and foreign bodies.
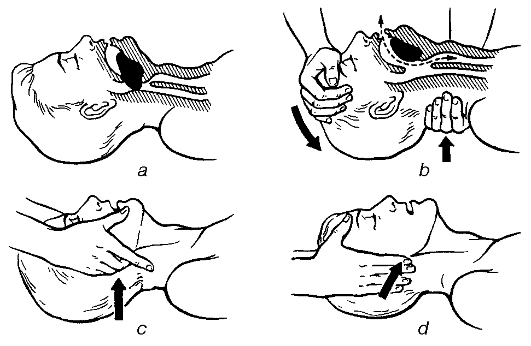
Fig. 19. Prevention of the tongue from falling back: a - the tongue has fallen back; b - prevention by extending the patient's head back; c - prevention by pulling forward the patient's mandible. Stage II (institution of artificial ventilation). This step is achieved through the methods of «mouth to mouth», «mouth to nose», and «mouth to mouth to nose» ventilation (fig. 20). To perform artificial ventilation the one doing it stands by the side of the patient (if the affected person is lying on the floor he has to kneel down) one hand is placed under the neck, the other on the forehead fixing the head in the maximum tilted position, the 1st and 2nd fingers are used to close tight the patient's nostrils, and with the mouth firmly fixed on the patients mouth he/she strongly breaths out into him. The patient is then left for a moment to allow a passive exhalation. The volume of air that is exhaled into the patient at a time is between 500 to 700 ml, breathing rate being 12 min-1. The effectiveness of artificial ventilation is assessed based on the excursion of the chest wall - rising on inhalation and falling on exhalation. When there is injury to the lower jaw or when the jaw is hanging too loose, artificial ventilation is done by «mouth to nose». To do this the hand is placed on the forehead, the head is fixed in the tilted position, and the other hand is used to firmly push the lower jaw against the upper, closing the mouth tightly. The patient's nose is grabbed by the lips and breathed forcibly into it. In newly born babies artificial ventilation is done by «mouth to mouth and to nose». The head of the neonate is thrown back. The health care provider uses the mouth to grab both the mouth and nose of the baby and breaths out into them. The respiratory volume of a newly born baby is 30 ml, breathing rate - 25-30 min-1. The abovementioned method of artificial ventilation should be performed through a gauze or handkerchief to protect the saver from acquiring a respiratory infection. For the same reason artificial ventilation can be performed using an S-shaped tube which is allowed to apply only by medical personnel (fig. 21). The bent tube keeps the root of the tongue from falling back, thus preventing airway obstruction. The S-shaped tube is inserted into the mouth by the bent side with the end upwards, and pushed along the lower edge of the upper jaw. At the level of the root of the tongue it is turned by 180°. The cuff of the tube firmly closes the patient's mouth, and the hand is used to close the nose. Breathing is done into the free lumen of the tube. Artificial ventilation can also be performed using a facemask or a reservoir bag. The mask is placed on the patient's face covering the nose and mouth.
Fig. 20. Mechanical ventilation: a - mouth-to-mouth mode; b - mouth-to-nose mode; c - mouth-to-mouth and nose mode; d - using an airway.
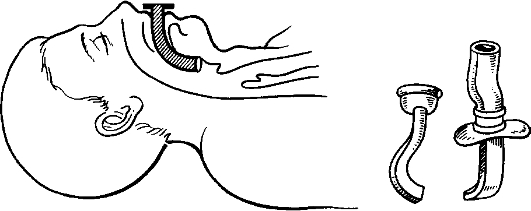
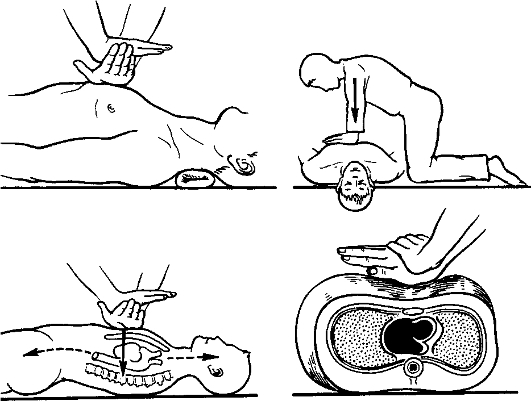
Fig. 21. Prevention of mechanic asphyxia using in airway. The narrow nasal part of the mask has to be fixed by the thumb, using three fingers (3rd, 4th and 5th), the lower jaw is raised and the 2nd finger is used to fix the lower part of the mask. At the same time the head is fixed in the tilted position backwards. The free hand is used to rhythmically press on the bag to produce an inhalation, passive exhalation occurs through special valves into the atmosphere. Oxygen can also be supplied through the bag. Stage III (closed chest massage). By this procedure one performs heart massage. Cardiac compression creates an artificial heart pump that can maintain the circulation. Blood supply to vital organs (the brain, heart, lungs, liver and kidneys) is thus restored. There are two types of cardiac massage - a closed chest, or an indirect, one and an open chest, or a direct one. Closed chest (indirect) cardiac massage is normally done before the patient arrives at the hospital; this involves rhythmic compression of the chest between the sternum and the spine. The manipulation is preferably performed with the patient lying on a hard surface. The hands are placed on each other at the right angle on the lower third of the chest, 2 cm off the point where the xyphoid process is fixed to the sternum (fig. 22). As the sternum is being pressed on with a force of about 8-9 kg, it is pushed towards the spine for about 4-5 cm. Cardiac massage is carried out continuously and rhythmically with the sternum being pressed on with the arms straightened at a rate of 60 pressings per minute. In children under 10 years of age heart massage is done using one hand at a rate of 80 pressings per minute, while in neonates it is performed using two fingers (the 2nd and 3rd ones), placed parallel to the sagittal plane of the sternum, at a rate of 120 pressings per minute. Open (direct) heart massage is applied in chest surgery, chest injuries or in chest rigidity that precludes adequate external massage. To perform open heart massage, one is to open the thoracic cavity at the 4th left intercostal space. The hand is then introduced into the chest, with four fingers put under the heart and the thumb lying on the top. The heart is massaged by pressing it rhythmically. When the chest is open enough, this can be done using both hands. Moreover, heart tamponade requires that the pericardium be opened.
Fig. 22. Position of the hands for an indirect cardiac massage. Resuscitation can be done by either one or two persons (fig. 23). If resuscitation is performed by a single person, he/she stands beside the patient. After cardiac arrest has been diagnosed and the oral cavity evacuated, four exhalations into the lungs are made using the «mouth to mouth» or «mouth to nose» ventilation. Afterwards, fifteen pressings of the chest alternate with two blows into the lung.
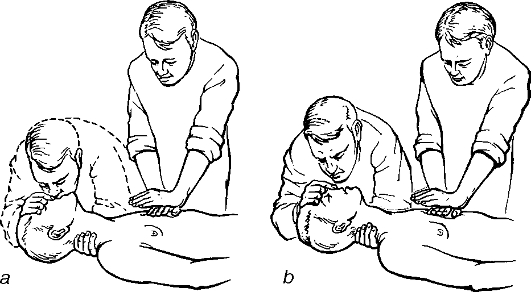
Fig. 23. Cardiopulmonary resuscitation: a - using a single hand and b - by two persons. If two persons are involved in the manipulation, they usually stand beside the patient unilaterally. One of them is to be responsible for heart massaging, while the other performs the artificial ventilation. The ratio of artificial ventilation to heart massage is 1: 5, i.e. one blow into the lungs is given following each fifth pressing on the sternum. The one involved in artificial ventilation checks for the carotid pulse, sees to it that the massage is being done correctly and also monitors the pupils. The two people performing the manipulation have to periodically interchange their positions. Resuscitation of the neonate is often done by a single person who periodically makes three blows into the lungs followed by fifteen pressing on the sternum. The adequacy of resuscitation is ascertained by constriction of the pupils with restoration of their reaction to light and the presence of a corneal reflex, hence the need for continuous monitoring the pupils. Heart massage is suspended every 2-3 minutes to check whether the heart has started beating on its own by feeling the carotid pulse. The moment it does, the massage should be stopped, while the artificial ventilation is continued. Stage IV (differential diagnosis, drug therapy, and heart defibrillation). This is performed by only intensive care physicians and involves such measures as electrocardiography, intracardiac drug injection and heart defibrillation. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 111; Нарушение авторского права страницы