|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Preparing the patient for general anaesthesia
The anaesthetist is directly involved in preparing the patient for anaesthesia and operation. The patient should be examined before the operation, history is taken not only of the principal disease that has necessitated the operation, but the details of concurrent conditions as well. If the surgery is scheduled, the patient should be treated of other ailments, and sanitation of the oral cavity should be done. The surgeon has to examine and assess the psychological status of the patient and exclude any possible allergies, previous operations, if any, and the anaesthesia used. Features of the face, the chest, the type of neck, the nutritive status are evaluated. All these are essential in making the right choice of anaesthesia and the anaesthetic. An important measure in preparation of the patient for general anaesthesia is evacuation of the gastrointestinal contents (gastric lavage, cleansing enema). To suppress the emotional reactions of the patient and depress the functions of the vagus preoperatively, specific preparations (premedication) are used. The patient is given sedatives on the eve of the surgery at night; tranquilizers (seduxen, relanium) are given to patients with neurotic reactions on the day before surgery. 40 minutes prior to the operation a narcotic analgesic is given subcutaneosly or intramuscularly: 1 ml of 1-2% promedol or 1 ml of lexir, 2 ml of fentanyl are given. To inhibit the vagus and reduce salivation 0, 5 ml of 0, 1% atropine are given. Patients with allergic conditions are in addition given an antihistamine drug. Immediately before the operation the mouth is inspected and removable teeth prosthesis are taken out. In emergency, gastric lavage is done and the premedication is given when the patient is on the operating table, the narcotic is given intravenously. Inhalation general anaesthesia using vapour and gaseous substances is achieved with special apparatus - anaesthetic machine (fig. 17). The main parts of the machine are as follows: 1) cylinder for the gaseous substances (oxygen, nitrous oxide and cyclopropane); 2) vaporiser for steam forming narcotic substances (ether, halothane, pentran); 3) dosimeter; 4) breathing contour. Oxygen is kept in blue cylinders under the pressure of 150 atmospheres. To reduce the outgoing pressures of nitrous oxide and oxygen, special reducers are used, which bring down the pressure to as low as 3-4 atmospheres. Kept under a lower pressure, cyclopropane can be given directly into the anaesthetic machine.
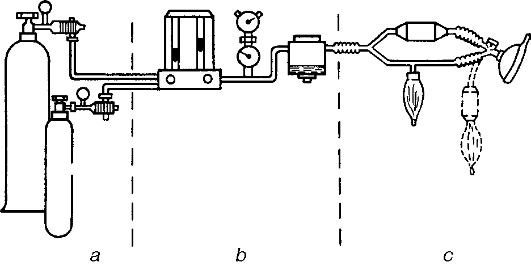
Fig. 17. Anaesthetic machine. a - gas bags; b - dosimeters and evaporators; c - ventilators. Vaporisers are necessary for steam forming narcotic substances. Steams of the narcotic are directed through a valve into the contour of the machine, concentration of the steam varies with the surrounding temperature. Dosage is not precise in arbitrary units, especially that of ether whose boiling temperature is 35, 6 °C. Nowadays, vaporisers with thermic compensators are widely used, which allows for a more precise dosage of the narcotic (in their percentage volumes). Dosimeters are meant for accurate dosage of gaseous anaesthetic drug and oxygen. Rotational dosimeters are often used - the float type. The stream of gas inside the gas tube directs upwards from below. The float dislocation is equal to the amount of gas used in litres per minute. Breathing contour comprise a breathing bellows (or mechanical ventilator), bag, hose, valves and absorbers. The anaesthetic substance passes through the breathing contour from the vaporijer and dosimeter to the patient, and then through the air-way out - into the machine. There are 4 types of breathing contours: open, partly open, closed and partly closed. The partly closed type is most often used, here inhalation is received from within the machine and exhalation is done partly into the machine and partly into the atmosphere. Exhaled air enters the machine and is purified of its carbon dioxide when it passes through the chemical absorbent. Inhalation anaesthesia can be achieved using the mask, endotracheal or endobronchial methods. The anaesthetic machine is first put in working condition as follows: 1) open the regulators of the nitrous oxide and oxygen cylinders; 2) check for the presence of gas in the cylinders by the reading on the manometer; 3) connect cylinders to the machine using the tubes; 4) if the anaesthetic drug is a volatile substance (ether, halothane, methoxyflurane), they are poured into the vaporijer; 5) fill the absorber with the chemical absorbent; 6) earth the machine; 7) make sure the machine is airtight. To use the mask method for general anaesthesia, the anaesthesist stands beside the patient's head to place the facemask on his/her face. A special belt is passed across the head to fix the mask on the face. If it is held manually, it should firmly be pressed to the face. The patient breathes in several times through the mask which is then connected to the machine. Oxygen is given to breathe for 1-2 minutes before the anaesthetic substance is allowed to flow. The dosage of the anaesthetic substance is slowly increased. Simultaneously, oxygen is given at the minimum rate of 1liter per minute. The anaesthetist constantly checks the patient's condition and flow of the anaesthetic. The nurse should permanently check the pulse and blood pressure. The anaesthetist examines the position of the eyeballs and the pupils, checks corneal reflex as well as the breathing pattern. When the surgical stage is attained, no more anaesthetic substance is given. Each patient is examined to determine the individual percentage volume dose of the anaesthetic required for at least the first level of the surgical stage of anaesthesia. If anaesthesia has been deepened to the third level of the surgical stage, the lower jaw has to be withdrawn. To do this, the thumbs are used to press on the angles of the lower jaw and pulled forward, until the lower incisors are placed forward to the upper ones. The 3rd, 4th and 5th fingers are then used to hold the lower jaw in that position. To prevent the jaw from falling back, airwaytubes can be used, these are kept to the root of the tongue to prevent it from falling back. It is noteworthy that giving anaesthesia at the third level of the surgical stage is dangerous in terms of overdose. At the end of the operation, after the anaesthetic drug has been put off, the patient continues to receive oxygen for some time before the mask is removed from the face. After the end of work with the machine, all the ventilators of the anaesthetic and cylinders are closed. The remaining volatile substances are poured out of the vaporijer. The tubes and bag of the anaesthetic machine are removed and sterilized in an antiseptic solution. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 118; Нарушение авторского права страницы