|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Tuberculous gonitis (tuberculous destruction of the knee joint).
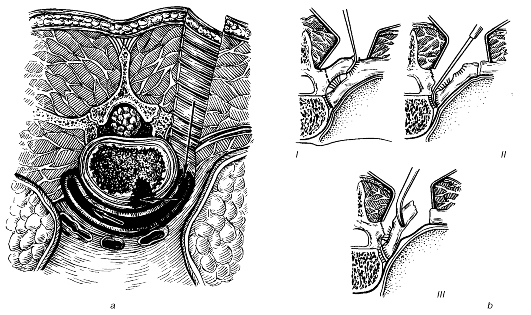
A. Epidemiology. • Young children are most commonly affected. • It accounts for 15-20% of cases of osseous and articular TB. B. The clinical course. Stage 1 - prearthritic - the disease is localized in the epiphyses: • the syndrome of tuberculous intoxication; • functional disorders of the limb involved (the patient is lame in his/her leg affected and easily gets tired); • no pain. Stage 2 - arthritic - the process spreads to the joint: • arthralgia due to an increase in joint size; • sleek skin overlying the joint affected; • loss of joint shape (it becomes fusiform); • the " balloting patella" sign (i.e. the patella sinks on pressing and assumes its initial position immediately when it is released); • half-bent leg; • purulent fistulae with discharge of small particles of bone sequestra (uncommon); • enlarged circumference of the joint affected and reduced circumference of the thigh on the limb involved as compared to that of the intact one; • a thicker skin fold on the lateral surface of the limb affected than that of the intact one (Alex-androv's sign). X-ray image demonstrates: • osteoporosis of the bones at the joint ends; • narrowed joint space; • destruction of the joint ends of the bones (in advanced cases). Tuberculosis of the bones of the fingers and toes (spina ventosa) A. Epidemiology: — children of the first year of life are commonly affected. B. Clinical picture: — pain in the hyperaemic fingers, which gets worse on moving; — Fusiform and oedematous finger. X-ray films show: • osteoporosis with marked periosteal changes in the phalanges. Treatment of TB involves both conservative and surgical methods. Of great importance are such supportive measures as nutrition with adequate amounts of protein, vitamins, trace elements as well as resort treatment. Antibacterial chemotherapy requires the use of specific antituberculous antibiotics (e.g. PASA, isoniazid). The affected organ must be immobilised from the very beginning, which prevents bone deformation and favours healing. For this purpose, splints, POP jackets and dressings are applied. The patient is allowed to walk about after the process has subsided. In tuberculous spondylitis it is advisable to wear a POP jacket for several years. Surgery is one of the major modalities in complex management of bone and joint TB. Radical operation: • necrectomy, or the excision of peri-articular tuberculous foci from the vertebral bodies and the bone epiphyses; • bone resection, or the removal of the joint ends of bones destructed (fig. 124, 125). Ancillary operation: • arthrodesis (i.e. forming artificial ankylosis), or the immobilisation of the joint, especially in the case of tuberculous spondylitis (spondylodesis) when the vertebral column is fixed using bone transplants or metallic constructions;
Fig. 124. Approach to the cervical vertebral bodies: a - costotransversectomy; b - costotransversectomy: steps I-III.
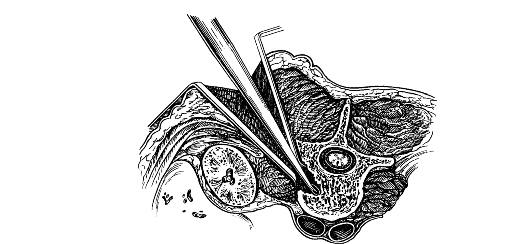
Fig. 125. Approach to the lumbar spine, debridement of the lumbar vertebral body. • laminectomy is indicated in compression of the spinal cord. Reconstructive opeartion: • osteotomy and joint trepanation to restore the organ's (limb, joint, spine) function after the inflammation has been eliminated. |
Последнее изменение этой страницы: 2019-06-08; Просмотров: 87; Нарушение авторского права страницы