|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
|
|
Архитектура Аудит Военная наука Иностранные языки Медицина Металлургия Метрология Образование Политология Производство Психология Стандартизация Технологии |
Federal Agency of EducationСтр 1 из 22Следующая ⇒
Federal Agency of Education TAMBOV STATE UNIVERSITY NAMED AFTER G.R. DERZHAVIN
А.V. Gulin S.E. Sinyutina А.G. Shubina
Biochemistry (part I)
Approved by the editors committee of TSU named after G.R. Derzhavin as a course book for foreign students studying medicine Speciality 060101 – Medicine
Tambov 2012 Editors: M.D., professor V.B. Maximenko M.D., professor K.I. Zasyadko
Contents I. THEORETICAL PART The subject of biological chemistry 1. Chemistry of proteins 1.1. Methods of exctraction and purification of proteins 1.2. Functions of proteins 1.3. Amino acid composition of proteins 1.4. The structural organisation of proteins 1.5. Physical and chemical properties of proteins 1.6. Classification of proteins 1.6.1. Simple proteins 1.6.2. Conjugative proteins 2. Enzymes 2.1. The chemical nature of enzymes 2.2. The mechanism of enzymes action 2.3. Kinetics of enzymatic reactions 2.4. Properties of f enzymes 2.5. Regulation of enzymes activity 2.6. Classification and nomenclature of enzymes 2.7. Enzymes in medicine 3. Vitamins 3.1. Fat soluble vitamins 3.2. Water soluble vitamins 4. Basic principles of biomembranes' organization 4.1. Structure and functions of membranes 4.2. Transport of substances across membranes 5. Transmembrane transduction of hormonal signal 6. Introduction to metabolism 6.1. Stages of catabolism 6.2. Bioenergetics 6.3. Organization and operation of respiratory chain 6.4. Uncoupling of oxidation and phosphorylation 6.5. Generation of free radicals in cells 6.6. Reactions of the common catabolic pathway 6.6.1. Oxidative decarboxylation of pyruvate 6.6.2. Citric acid cycle 7. Carbohydrates metabolism 7.2. Glycogen metabolism 7.3. Glycolysis 7.4. The inclusion of glucose and galactose in glycolysis 7.5. The shuttle mechanisms 7.6. Cori cycle 7.7. Alcohol fermentation 7.8. Pentose-phosphate pathway (hexose monophosphate shunt) 7.9. Gluconeogenesis 7.10. Regulation of carbohydrates metabolism 7.11. Violations of carbohydrate metabolism II. LABORATORY PRACTICE Laboratory work 1. The analysis of amino acids and proteins Laboratory work 2.Complex proteins: phosphoproteins and glycoproteins Laboratory work 3. Complex proteins: nucleoproteins and chromoproteins Laboratory work 4. Enzymes Laboratory work 5.Identifying of enzymes activity Laboratory work 6. Vitamins Laboratory work 7. Oxidoreductases Laboratory work 8. Carbohydrates metabolism Bibliography I. THEORETICAL PART The SUBJECT Of BIOLOGICAL CHEMISTRY Biochemistry is a science about chemical bases of processes of vital activity, studying chemical components of living cells, and also reactions and processes in which they participate. Its main task is the establishment of communication between a molecular structure and biological function of chemical components of living organisms. The subject of medical biochemistry is the chemical processes occurring in a human body in norm and pathology, diagnostics and forecast on the basis of biochemical researches. CHEMISTRY OF PROTEINS Proteins are high-molecular nitrogen-containing organic compounds, which molecules are constructed of amino acids residues. Amino acid units linked together with peptide bonds. Proteins compound the basis of both frames and functions of live organisms. Natural proteins are constructed of 20 various amino acids. These amino acids can be combined in the most different sequences, therefore they can form about millions various proteins. They provide existence of about thousand different living organisms, ranging from viruses to humans. Each organism is characterized by a unique number of proteins. The content of proteins in various tissues of one organism is unequal. So, in a human body there are proteins in % from dry weight: in muscles - 80, in brain - 45, in bones - 20. Element composition of proteins in terms of dry weight: C - 50-54 %; Н - 6, 5-7, 3 %; O - 21-23 %; N - 15-17 %; S - up to 0, 5 %. As a part some proteins contain in small amounts phosphorus, iron, manganese, magnesium, iodine, etc. The amount of nitrogen is rather constant in all proteins (about 16 %), therefore it is possible to define the quantity of protein in biological objects by the protein nitrogen. FUNCTIONS OF PROTEINS Catalytic function. The majority of enzymes known as biological catalists, are proteins. Now, some thousand enzymes are described. Transport function. Respiratory function of blood, in particular oxygen transfer, is carried out by molecules of hemoglobin protein of erythrocytes. Albumins of blood serum take part in transport of lipids. Protective function. In response to bacteria, toxins, viruses or alien proteins entering in organism protective proteins-antibodies are synthesized (immune defenses). A number of proteins of blood plasma are capable to coagulation that protects from wounds blood loss (physical protection). Hormonal function. A series of hormones is presented by proteins or polypeptides, for example, pancreas hormone - insulin. Structural function. In complex with lipids proteins participate in the formation of biomembranes of cells. Cytoskeleton structural proteins provide shape of cells and many organoids. Structural proteins are collagen in connective tissue, keratin in hair, nails, skin, elastin in a vascular wall, etc. Nutrient (reserve) function. Proteins of egg (ovalbumins) are a source of nutrition for the fetus. The basic protein of milk (casein) also carries out nutrient function. Receptor function. Protein receptors can be integrated into the cell membrane or in the cytoplasm. The receptor accepts a signal which is often a chemical substance. Contractile (motor) function. Contractile function is inherent to muscular proteins (actin and myosin), to proteins of cytoskeleton and that provides discrepancy of chromosomes in the course of mitosis. Other important functions of proteins - ability to sustain oncotic pressure in cells and blood, the buffer properties sustaining physiological рН value of internal environment, etc. CLASSIFICATION OF PROTEINS Depending on chemical composition proteins are divided into 2 groups. Simple proteins are constructed of the amino acids residues and in hydrolysis give only free amino acids. Conjugative proteins are two component proteins which consist of simple protein and non-protein component ( prosthetic group ). SIMPLE PROTEINS Albumins and globulins. Albumins are simple proteins; are a part of animal and vegetative tissues; are contained in eggs, blood serum, milk, in seeds of plants. They are soluble in water, salting liquids, acids and alkalis. Approximately 75-80 % of osmotic pressure of proteins of blood serum are albumins; their one more function - transport of fat acids. Globulins are group of animal and plant proteins widely spread in nature. They are globular proteins. They are soluble in weak solutions of neutral salts, weak acids and alkalis. The globulins presented by a-fraction are contained in blood in a complex with bilirubin and with lipoproteins of high density. The fraction of β -globulins includes a prothrombin which is the precursor of thrombin - the protein participating in blood coagulation. The fraction of g-globulins is the most heterogenous. The major g-globulins are immunoglobulins. The ratio albumin/globulin has a diagnostic importance: in norm it is close to 2, and during inflammatory diseases it is decreases. Protamines and histones. Protamines are low molecular weight proteins in nuclei of spermatozoons of fishes and birds. They contain 60-85% arginine and possess the basic properties. They are well dissolve in water, acid and neutral medium and precipitate in alkalis. In nuclei of cells they associate with DNA. Histones are small proteins of the basic character. Their composition has lysine and arginine which amount does not exceed 20-30%. There are five various types of histones: H1, H2A, H2B, H3 and H4. These proteins are mainly in nuclei of cells. They take part in the structural organization of chromatin. Prolamins and glutelins. Prolamins are proteins of vegetative origin. They contain 20-25% of glutamic acid and 10-15% of proline. They are dissoluble in 60-80% ethanol water solution while all other simple proteins in these conditions usually form sediment. Glutelins are simple proteins. They are contained in seeds of gramen, in green parts of plants. They are characterized by high amount of glutamic acid and lysine. They are dissoluble in dilute solutions of alkalis. Glutelins are reserve proteins. CONJUGATIVE PROTEINS Conjugated proteins are two-component proteins which consist of simple protein and non-protein component ( prosthetic group ). 1. Chromoproteins (from Gr. chroma - color) consist of simple protein and the pigmented non-protein component bound to it. We distinguish hemoproteins and flavoproteins. They participate in such processes as breath, transport of oxygen and carbon dioxide, redox reactions, light- and colour perception, etc. The group of hemoproteins include hemoglobin, myoglobin, cytochromes, catalase, peroxidases. All of them contain ferriporphyrin, but vary in protein structure, and carry out various biological functions. Specific distinctions of hemoglobin are caused by globin. Let's consider hemoglobin structure. It is a blood protein. Non-protein component of hemoglobin is the heme (fig. 5). It’s a pigment giving blood its red color. The basis of its structure is the protoporphyrin IX. In the heme centre the atom of iron is bounded to two atoms of nitrogen covalently and with two others by coordination bonds. A heme is " wrapped up" by one polypeptide chain. In a molecule of hemoglobin of an adult person НbА there are four polypeptide chains which together form the protein part of a molecule - globin. Two α -chains contain 141 amino-acid residues, two β -chains – 146 (fig. 6).
Fig. 5. Heme Fig. 6. Hemoglobin In blood of an adult person there is also hemoglobin НbА2 (2α, 2δ chains, 2, 5%) and НbA3 (less than 1%, differs by structure of b-chains). There is fetal hemoglobin HbF, consisting of 2 α - and 2 γ -chains. Hemoglobin F possesses the increased affinity to oxygen and allows rather small volume of blood of a fetus to carry out oxygen-bearing functions more effectively. Blood of the newborn contains up to 80% HbF, by the end of the 1st year of life it is almost entirely changed to НbА. Diseases of hemoglobins (more than 200) are called hemoglobinoses. 1. Hemoglobinopathy, at the basis of which hereditary structural change of any chain of normal hemoglobin. In blood of a human about 150 various types of mutant hemoglobins are found. Abnormal hemoglobins differ in physical and chemical properties (electrophoretic mobility, solubility, isoelectric point, affinity to oxygen). Classical example of hemoglobinopathy is sickle-cell anemia. It widely spread in the countries of South America, Africa and South East Asia. Chemical defect is reduced to glutamic acid changing in 6th position from the N-end to valine in β -chains of a molecule of hemoglobin (HbS). It is the result of a mutation in DNA molecule. The HbS solubility and affinity to oxygen are reduced. Erythrocytes in the conditions of low partial pressure of oxygen take the form of a sickle. HbS after oxygen return in tissues turns in low solubility desoxiform and drops out into sediment in the form of spindle-shaped crystals. They distort a cell and lead to a hemolysis. The heterozygous form of anomaly proceeds asymptomatically or is accompanied by an easy hemolytic anemia. Homozygous individuals from the first months of life have the heavy form of sickle-cell anemia. Disease proceeds sharply, and children often die in an early age. 2. Thalassemia is a group of diseases with hereditary infringement of synthesis of one of globin chains. We distinguish α - and β -thalassemia. Hemoglobinopathy Н is one of the variants of a-thalassemia. It manifests in hemolytic anemia, the precipitation of hemoglobin H, enlarged spleen, severe osteal changes. 3. Iron-deficient anemia is infringement of synthesis of hemoglobin owing to deficiency of iron. Principal causes are blood loss and lack of nutrition rich with heme - meat and fish. Hemoglobin derivatives Oxyhemoglobin HbO2. Molecular oxygen is joined to each heme of Hb by means of iron coordination bonds. Binding of each molecule of oxygen facilitates binding of the subsequent. This allosteric dependence has received the name Bohr effect. Oxyhemoglobin, getting to tissues, loses oxygen, becoming deoxyhemoglobin. Carbhemoglobin HbCO2 is hemoglobin bond with carbon dioxide. It is unstable and quickly dissociates in pulmonary capillars detaching СО2. Carboxyhemoglobin HbCO is a product of the addition of carbon monoxide to hemoglobin. Hemoglobin has high affinity to CO and is strong bound with it. Hemoglobin loses ability to bind oxygen, and here comes death from suffocation. Methemoglobin MtHb is the hemoglobin form in which heme iron is in a trivalent state. It is not capable to carry oxygen. It is formed of free hemoglobin under the influence of various oxidants, and in an organism - after some poisonings. Methemoglobinemia is an appearance of methemoglobin in blood. There are hereditary and acquired methemoglobinemia. Hereditary evolves as a result of presence of abnormal hemoglobins. Among the acquired can be toxic methemoglobinemia of exogenous parentage, arising under the influence of some chemicals (nitrates, nitrites, aniline, some medical products), and endogenous, owing to infringement of production and adsorptions of nitrates during enterocolitis. With significant methemoglobinemia there is an anoxemia (hypoxia). Method of qualitative test of various derivatives of hemoglobin is research of their absorption spectrums. Myoglobin is a globular protein which reserves in muscles molecular oxygen and transfers it to the oxidative systems of cells. It consists of one polypeptide chain. As well as in hemoglobin, the active centre of a molecule binding O2, is the heme. Myoglobin defines the color of muscles. Chromoproteins are also catalase, peroxidase, cytochromes enzymes. Flavoproteins are the chromoproteins, which prosthetic groups are presented by derivatives of isoalloxasine - flavine mononucleotide (FMN) and flavine adenine dinucleotide (FAD). Flavoproteins are a part of some oxidoreductases - enzymes catalyzing redox reactions in a cell. 2. Lipoproteins consist of protein and the prosthetic group presented by any lipid (neutral fats, free fatty acids, phospholipids, derivatives of cholesterol). Lipoproteins are widely spread and also carry out various biological functions. Representatives of lipoproteins are protein of lungs tissue, lipovitellin of an egg yolk etc. Lipoproteins are present in free state (mainly in blood plasma). Lipoproteins of blood serum contain hydrophobic lipid nuclei surrounded with polar lipids and a cover of proteins, called apoproteins. They provide transport of water insoluble lipids. The lipids covalently bound with protein, serve as an anchor with the help of which proteins are attached to the membrane. These are structured lipoproteins (lipids of cells membranes, myelin sheath of nerve fibers). 3. Phosphoproteins are conjugative proteins into which composition as a non-protein component the phosphoric acid enters and is attached to a polypeptide chain by an ester bond through the residues of serine or threonine. The ionic bonding is also possible. Phosphoproteins include caseinogens of milk, egg white ovalbumin, a number of enzymes such as RNA polymerase. A large number of phosphoproteins found in cells of the CNS. Phosphoproteins are a valuable source of energy and plastic material in the process of embryogenesis and postnatal growth and development, participate in the regulation of nuclear activity of the cell, ion transport and oxidative processes in mitochondria. 4. Glycoproteins are conjugative proteins that contain, in addition to a simple protein or peptide, linear or branched geterooligosaccharide chains containing from 2 to 15 residues of hexose, pentose and the terminal carbohydrate (N-acetylgalactosamine or others). Carbohydrate component is connected to the protein by covalent bonds – N-glycoside and O-glycoside. Glycoproteins are proteins of blood plasma (except albumin), certain enzymes, saliva mucin, proteins of cartilage and bone tissues. Glycoproteins are important structural component of cell membranes. They provide a cell adhesion, molecular and cellular recognition. Carbohydrate components in addition to the informative function increase the stability of the molecules, to which they belong, to various chemical or physical treatments, and protect them from the action of proteases. Erythrocyte membrane glycoproteins determine the blood group in humans. The typical glycoproteins include interferons, immunoglobulins. Interferons - inhibitors of reproduction of many types of viruses. They are formed in the cell in response to the invasion of viruses’ nucleic acids. Interferons are proteins thought to be essential not only as protective against viral infection, but also of tumors. Immunoglobulins, or antibodies are protective proteins. They neutralize entering the body foreign substances of any chemical nature - antigens. There are three major classes of immunoglobulins: IgG, IgA, IgM; minor classes of immunoglobulins of human plasma are referred to as IgD and IgE. Immunoglobulins of different classes differ in molecular weight, the concentration in the blood, biological properties. At rheumatic arthritis abnormal antibodies are synthesized with an unusually short sugar chains, which causes stimulation of the immune system against the organism. Proteoglycans are complexes of proteins and glycosaminoglycans. Carbohydrate in these compounds is the main part of the molecule (95%). Typical glycosaminoglycan is hyaluronic acid. Its main function in the connective tissue is binding of water. Heparin involved in the regulation of blood coagulation. 5. Metalloproteins, in addition to protein, contain ions of a single metal or several metals. NUCLEIC ACIDS Nucleic acids – RNA and DNA – are polymers of nucleotides. DNA is found in the cell nucleus and mitochondria. RNA is found in all parts of the cell. We distinguish messenger RNA (mRNA). It synthesized by DNA and determines the order of amino acids in a protein molecule. Ribosomal RNA (r-RNA) is part of the ribosome. Transport RNA (t-RNA) carries amino acids to the place of protein synthesis. NA provide storage and transmission of genetic information by programming the synthesis of cellular proteins. Bases of NA – DNA: purine - A, G, pyrimidine – C, T; RNA: purine – A, G, pyrimidine – C, U. One of the important properties of free nitrogenous bases is that they can exist in two tautomeric forms. Also NA containe carbohydrates (ribose and deoxyribose) and phosphoric acid residues. Nucleotides consist of three components: a pyrimidine or purine base, a pentose and phosphoric acid (fig. 7). Nucleotides are nucleoside phosphates.
To study the chemical composition of NA using sequencing - splitting up into fragments by enzymes or chemical reagents. Products are analyzed by electrophoresis, chromatography, etc. DNA isolated from different tissues of the same species, has the same composition of the nitrogenous bases. Analysis of DNA composition and the quantity of bases was established for the first time by Erwin Chargaff, Austrian-born American biochemist. The quantitative relations were named Chargaff's rules. 1. The quantity of purine bases (in moles) is equal to the quantity of pyrimidine bases: A + G = C + T. 2. The quantity of adenine and cytosine is equal to the quantity of guanine and thymine: A + C = G + T. 3. The quantity of adenine is always approximately equal to that of thymine, and the quantity of guanine is always approximately equal to that of cytosine. A = T, G = C. 4. The A/G ratio varies widely from species to species. The coefficient of specificity is (G + C) / (A + T) (0, 54 - 0, 94 in animals, 0, 45-2, 57 in microorganisms). Test Questions 1. Give a characteristic of amino acids as structural monomers of proteins. What are the features of the peptide bond formation? 2. Give a definition of the primary structure of protein. What is the determining role of primary structure in the formation of higher levels of organization of the protein molecule? 3. What links stabilize the secondary structure of protein? What types of secondary protein structure are you know? 4. What is meant by the tertiary structure of protein? What types of bonds stabilize it? 5. Give a characteristic of quaternary structure of proteins. What are the monomers and oligomers? 6. What is the relationship of structure and function of proteins? 7. Name the major functions of proteins in the body. 8. What methods can determine the molecular weight of protein? 9. Does the solubility of proteins depend from their amino acid composition? 10. What is meant by denaturation and renaturation of proteins? Which agents cause denaturation? 11. What is the isoelectric point of proteins? 12. How is the process of salting out of proteins use in medicine? 13. Name the functions of albumin and globulins of blood plasma. 14. Give examples of fibrous proteins. 15. Give the classification of complex proteins. 16. Consider the structure and function of hemoglobin A. ENZYMES Enzymes are substances mainly of protein nature, which have catalytic activity. The phenomena of fermentation and digestion have long been known. The term " enzyme" goes from the Greek En zyme - in yeast, as well as the " ferment" from Lat. Fermentatio - fermentation. The science that studies the enzymes is called enzymology. Although laboratory synthesis of several enzymes has carried out (ribonuclease, lysozyme), the only way to get enzymes is their excretion from biological objects. ENZYME PROPERTIES Enzymes differ from the usual catalysts with a number of properties. Heat-labile or heat-sensitive (fig. 13).
Fig. 13. Dependence of the enzymatic reaction velocity on temperature.
At temperatures below 45-50°C, the velocity of most biochemical reactions is increased twice when the temperature increase of 10°C (Vant Hoff's rule). At temperatures above 50°C a heat denaturation of the enzyme begins. It is greatly influenced the reaction rate and can lead to a complete cessation of the enzymatic process. The temperature, at which the catalytic activity of the enzyme is maximal, is called its temperature optimum. The temperature optimum for most enzymes of mammals is in the range 37-40°C. At low temperatures (0°C and below) enzymes are usually not destroyed, but their activity decreases to almost zero. The dependence of enzyme activity on the pH of the medium (fig. 14).
Fig. 14. Dependence of the enzymatic reaction velocity on pH. There is an optimum pH of the medium for each enzyme in which it shows maximum activity. pH optimum of the enzyme lies within a narrow zone of hydrogen ion concentration. It corresponds to physiological values of pH 6.0-8.0 which developed in the course of evolution. Exceptions are pepsin - 1.5-2.5; arginase - 9.5-10. According to modern concepts, the impact of changes in pH on the enzyme molecule is the impact on the tertiary structure of proteins. Enzyme specificity. The high specificity of enzyme action is due to the conformational and electrostatic complementarity between the substrate and enzyme molecules and the unique structural organization of the active site. The absolute specificity is the ability of the enzyme to catalyze a single reaction. Such enzymes are urease, arginase. Urease catalyzes the hydrolysis of urea to NH3 and CO2. Relative (group) specificity is the ability of the enzyme to catalyze a group of reactions of a certain type. Examples are peptidase, hydrolyzing peptide bonds in proteins and peptides. Stereospecificity is the ability of enzyme to catalyze the conversion of only one spatial isomer. The enzyme fumarase catalyzes the conversion only of trans-isomer of fumarate and has no effect on the cis-isomer maleic acid. The high specificity of the enzyme plays an important role in the regulation of metabolism, providing a high speed only to certain chemical reactions of all possible conversions.
Control of enzyme activity. Allosteric regulation. In many cases, the main type of regulation of multi-enzymatic process velocity is feedback inhibition. The final product inhibits the activity of an enzyme catalyzing the first stage of synthesis. The final product binds to the allosteric center of the enzyme, causing inhibition of the entire chain of synthetic reactions. This is feedback inhibition or end product inhibition.
ENZYMES IN MEDICINE Enzymes are used as therapeutic agents: - in their absence or deficiency (inherited or acquired); - for the specific destruction of some metabolic products.
Enzymes are used in the clinic as analytical reagents. Immobilized enzymes are often used for the analysis, which are artificially connected with the water-insoluble carrier, which increases the stability of protein catalysts.
Analysis of the kinetics of appearance and disappearance of enzymes in the serum is used in the diagnosis. The composition of enzymes and their tissue distribution in an adult is mainly constant and can change in diseases. Almost all of the enzymes of the organism are functioning intracellularly. When tissue is damaged intracellular enzymes appear in the serum. Such enzymes are called indicator enzymes. By the appearance of several tissue enzymes in plasma or serum in high amounts one can conclude on the functional status and lesions of various organs.
Enzimopathy (synonym fermentopathy ) is the common name of diseases, developing as a result of the absence or decreased activity of certain enzymes. As a result of the interdependence of metabolic pathways defect of a single enzyme often leads to a number of disorders in the metabolism. We distinguish hereditary and acquired enzymopathy. 1. Hereditary enzimopathys are associated with genetically determined deficiency of one or more enzymes. There are more than 150 hereditary enzymopathies, which are based on gene mutations. 2. Acquired enzimopathy. Toxic enzymopathy is a consequence of toxic effects of xenobiotics and environmental mutagens. Lead, which is contained in the transport exhaust fumes, causes a inhibition of the enzyme aminolevulinatdehydrase involved in the synthesis of heme, which manifests the development of anemia of children in the city. Nutritional enzymopathy may be due to prolonged lack of protein in the diet, vitamin deficiency, unbalanced nutrition. Test Questions 1. Describe the chemical nature and structure of enzymes. 2. What is the structure of the active center of enzyme? What is the allosteric center? 3. Give examples of isozymes; multimolecular enzyme systems. 4. On what basis enzymes are classified? 5. Describe the mechanism of enzyme action. 6. What is the difference between the theories of Fisher and Koshland? 7. How do changes in pH and temperature influence on the rate of enzymatic reactions? 8. What is meant by the specificity of enzyme action? 9. How is the regulation of enzyme activity done? 10. What types of enzymes inhibition do you know? 11. How can be carried out in practice the determination of the enzymes activity? 12. Give examples of the enzymes usage in medicine.
VITAMINS Vitamins (from Lat. vita - life) are organic compounds required in the diet in small amounts. They ensure the normal development of human and animal, and an adequate rate of occurrence of biochemical and physiological processes. Vitamins are the assembly group of organic compounds in the chemical and physical point of view. The physiological effects of vitamins are also very different. 100 years ago it was believed that for the normal life of the human organism flux of proteins, fats, carbohydrates, minerals and water is enough. Practice and experience have shown that there are specific diseases which development is directly related to malnutrition (scurvy, beriberi). The need for vitamins is negligible: approximately a person should consume daily 0.1 - 0.2 g. of vitamins. In many cases, vitamins are components of enzymes. Avitaminosis ( vitamin deficiency ) is a disease that occurs in the absence of food vitamins or in total violation of assimilation of any vitamin. Hypovitaminosis is insufficient intake of vitamins with food or their incomplete assimilation. Hypervitaminosis is pathological state associated with large quantities of vitamins in the organism. The causes of hypo- and avitaminosis in humans and animals are usually divided into exogenous and endogenous. An exogenous factor is insufficient intake of vitamins or their complete absence in the diet. Endogenous factors are: a) increased requirement for vitamins in certain physiological and pathological conditions (pregnancy, hyperthyroidism); b) violation of the process of absorption of vitamins in the digestive tract diseases; c) enhanced disruption of vitamins in the intestine due to the development of its flora; d) liver, pancreas diseases, accompanied by malabsorption of fat and therefore fat-soluble vitamins. The classification is currently used based on the solubility of the vitamins. FAT SOLUBLE VITAMINS Vitamin A ( retinol ). Vitamin A has several vitamers. Vitamer is a substance similar in chemical structure and having physiological effects characteristic of a particular vitamin. Retinol is oxidized in the organism with the participation of the biocatalyst. It is converted to retinal, also having the activity of vitamin A. Vitamin A affects the barrier function of skin, mucous membranes, the permeability of cell membranes and biosynthesis of glycoproteins, it is involved in light perception, being a part of the photosensitive pigment rhodopsin. Vitamin A deficiency leads to inhibition of growth, weight loss, lesions of skin, mucous membranes and eyes (night blindness). Vitamin A is found in liver, egg yolk, milk, oil; provitamin A (carotene) - in red pulp vegetables. Daily requirement is 2.7 mg. In humans body vitamin A is stored mostly in liver. There are cases of A hypervitaminosis at eating polar bear, seal, walrus liver, which contains plenty of vitamin A. Hypervitaminosis may develop as a result of receiving large amounts of fish oil and preparations with vitamin A. The characteristics of hypervitaminosis are eye inflammation, hair loss, headaches, dyspepsia (nausea, vomiting) dermatitis. Vitamin D (calciferol) in the human organism exists as a form of D2 and D3. Precursor of vitamin D2 (ergocalciferol) is ergosterol, which is present in plants. Precursor of vitamin D3 (cholecalciferol) is cholesterol, which is present in animals. Ergosterol and cholesterol are transformed into D2 and D3 under the influence of solar radiation. Calciferols are involved in the regulation of calcium and phosphorus digestion in the intestine, in osteogenesis, in the synthesis of mRNA and Ca-binding proteins and hormones. Vitamin D deficiency in children leads to rickets. The result is bone softening and deformation, thickening at the bone-cartilage boundary ribs, large head, enlarged abdomen due to the muscle hypotonia). D avitaminosis in adults leads to osteomalacia and osteoporosis. It is bone demineralisation, causing the bones become fragile. D hypervitaminosis is observed at very high dosages of vitamin and can be fatal. Toxic effect includes resorption of bones and deposition of phosphates in soft tissues (kidney and arteries). Vitamin D is found in animal products - butter, liver, egg yolk and oil. Daily requirement is 10 micrograms, for children - 20-25 microgramms. To prevent rickets in children UV irradiation is recommended. Vitamin E (tocopherol) (from the Greek Tokos - descendants, Fero - bring) got its name because it was established that it regulates the process of reproduction in rats. Vitamin E is one of the strongest natural antioxidants. It protects polyunsaturated fatty acids and lipids of cell membranes from oxidation, especially from peroxidation reactions. In the absence or deficiency of vitamin E in humans and animals embryogenesis is disturbed and degenerative changes in the reproductive organs are observed. Degeneration of the spinal cord develops and there is paralysis of limbs, fatty liver, muscular dystrophy, biochemical changes in muscles. Sources of Vitamin E are mainly vegetable oils, cabbage and grain products. It also contained in meat, milk, butter, eggs. Vitamin E is deposited in muscle, pancreas, so the development of avitaminosis is almost not observed. Daily requirement is 5 milligrams. Vitamin K (phyllochinone). It regulates the process of blood clotting. Vitamin K deficiency can lead to spontaneous nosebleeds, bloody vomiting and internal bleeding. K avitaminosis is rare. A mixed diet is rich enough with it; the intestinal micro flora is capable of synthesizing vitamin K. The drug " vikasol" is derived from vitamin К 3. WATER SOLUBLE VITAMINS Vitamin C (ascorbic acid) is colorless crystals with acidic taste. Ascorbic acid participates in the redox processes. It is involved in the synthesis of collagen, folic acid, adrenal hormones, and tryptophan. It is important in the breakdown of hemoglobin in tissues. Vitamin C enhances the synthesis of immunoglobulins. Deficiency of vitamin C leads to lessening of organism weight, weakness, shortness of breath, heart pain, decreasing of immunocompetence. In severe cases scurvy develops. The permeability and fragility of blood vessels increase. There are spontaneous hemorrhages, and loss of teeth. The basis for these phenomena is disorders of collagen synthesis. Source of vitamin C for humans are canker berry, black currants, mountain ash, red pepper, tomatoes, lemons, and cabbage. Daily requirement is 75 mg. Vitamin B1 (thiamine) is the first crystalline vitamin produced in the laboratory. It contains pyrimidine and thiazole rings having a methylene bridge. The active form of thiamine is thiamine pyrophosphate (TPP, or cocarboxylase). It is part of the five enzymes involved in intermediate metabolism. Usually it is decarboxylation reactions. TPP is connected with energy releasing reactions. Symptoms of avitaminosis В1 are disruption of the digestive system, mental disorders (hallucinations), degenerative changes in nerve endings and the vascular bundles, atrophy and paralysis of limbs, depression of the cardiovascular system. The В1-avitaminosis results in disease called (" beri-beri" polyneuritis), which can lead to paralysis and death. Sources of vitamin В1 are yeast, cereals, nuts, bread from meal, when the grain during processing does not lose the embryos and membranes. In animal products it is found in the liver, kidneys and brain. Daily requirement is 1.2 mg. Vitamin B2 (riboflavin). The basis of the riboflavin molecule is isoalloxazine, which combines benzene, pyrazine and pyrimidine rings. It is a substance of yellow color. The ability of riboflavin to be easily oxidized and restored is the basis of its biological effects. Riboflavin is a coenzyme of oxidoreductases (part of the FAD and FMN). Riboflavin deficiency lead to the stop of hair growth, loss of hair, dermatitis, mucous membranes damage (especially in the corners of the mouth), fatigability, decrease in working capacity, disruption of normal hemoglobin synthesis; muscular weakness. Sources of vitamin В2 are milk, meat, liver, kidney, eggs, yeast, green vegetables, cereals, fruits. Daily requirement is 1.7 mg. Vitamin В 6 (pyridoxine) is a derivative of 3-oxypyridine. It presents itself with pyridoxole, pyridoxal and pyridoxamine, all of them in the organism are able to transform to the pyridoxal phosphate, which participates in chemical reactions. Pyridoxal phosphate is the prosthetic group of carboxylases and transaminases involved in the formation of biogenic amines, transformation of amino acids, and synthesis of heme of hemoglobin. В6 deficiency disease involves violations of the metabolism of proteins and amino acids. The main symptoms are a violation of hematopoiesis and the development of various types of dermatitis that cannot undergo the treatment with nicotinic acid. В6-vitamin deficiency is also accompanied by violation of lipid metabolism that leads to the development of atherosclerosis. Sources of pyridoxine are beef, fish, peas, egg yolk and green parts of plants. Daily requirement is 2 mg. Since vitamin B6 is widely distributed in foods and can be partially synthesized by intestinal micro flora, in normal conditions, B6-deficiency disease in humans has not been observed. Vitamin B12 (cobalamin). It contains the grouping of four pyrrol rings with Co atom in the center. Derivatives of B12 coenzymes are composed of a number of enzymes that accelerate the most important reactions of nitrogen-containing compounds, carbohydrate, nucleic acid and lipid metabolism. B12 is involved in transmethylation reactions, intramolecular transfer of H atoms and various functional groups (hydroxyl, amine, etc.). With a lack of vitamin B12 disruption of hematopoiesis in bone marrow occurs, causing anemia malignant megablastic, disruption of the nervous system, reducing the acidity of gastric juice. Vitamin B12 is the only vitamin the synthesis of which is carried out only by microorganisms. Sources of cobalamin: meat, beef liver, fish, milk and eggs. Plants do not contain vitamin B12. Depot of vitamin B12 in humans is in the liver, where it accumulates in the amount of a few milligrams. Daily requirement is 3 micrograms. Vitamin B5 (pantothenic acid) is found in all animal, plant and microbial objects (Greek pantos - everywhere). Pantothenic acid is a part of coenzyme A. CoA is involved in transfer reactions of acyl groups. A number of biochemical reactions are associated with CoA that underlies the oxidation and fatty acid synthesis, the biosynthesis of fats, oxidation of breaking up products of carbohydrates. In the absence of vitamin B5 there can be dermatitis, slow growth, there is weight loss, hair loss and depigmentation of hair, degenerative changes in the nervous system. Discoordination of movements, paralysis, disruption of the gastrointestinal tract, reproductive organs and adrenal glands can be related to this. In humans, B5 vitamin deficiency is rare as pantothenic acid is produced by intestinal micro flora. Sources are yeast, milk, eggs, liver, kidneys, peas, cauliflower, potatoes, tomatoes. Daily requirement is 10 mg. Vitamin PP (nicotinic acid and nicotinamide, niacin, B3) is a derivative of pyridine. Vitamin PP is involved in all types of metabolism: carbohydrate, protein and lipid. Nicotinamide is a part of the most important coenzymes – NAD+ (nicotinamide adenine dinucleotide) and NADP+ (nicotinamide adenine dinucleotide phosphate), involved in redox reactions. Vitamin PP is necessary for energy production. Avitaminosis PP is expressed in an inflammation of the mucous membranes of the gastrointestinal tract, and then a skin inflammation (dermatitis) on the areas which are exposed to the sun irradiation. It is a pellagra disease. Also damage of the brain is observed. So, it is a disease of 3D: dermatitis, diarrhea, dementia. Sources of vitamin PP for humans are liver and kidneys of animals, yeast, buckwheat, beans, etc. A certain amount of nicotinic acid is synthesized in the human organism from the amino acid tryptophan. Daily requirement is 18 mg. Folic acid, vitamin Вс (pteroylglutamic acid). Вс vitamin deficiency is rare, because folic acid is synthesized by the micro flora of the gastrointestinal tract and always enters the organism in sufficient quantity, but in the case of this vitamin deficiency anemia and disorders of the digestive organs can occur. Folic acid, as a coenzyme of several enzymes, carries one-carbon fragments in the biosynthesis of many compounds: methyl group, oximethyl (-СН2ОН), formyl. Sources of folic acid are spinach, cauliflower, animal’s liver, bread. Particularly high content of it is in yeast. Vitamin P (rutin). Currently, there are many compounds with P-vitamin activity. They are called bioflavonoids. In the absence of vitamin P capillary permeability is increased, which is accompanied by bleeding, pain in the limbs, general weakness and fatigue. It is suggested that vitamins P are involved in redox reactions. Source of vitamin P for a human are the same products, in which there are a lot of vitamin C, such as black currant and lemon. Vitamin H (biotin). With a lack of this vitamin in humans there is inflammation of the skin, hair loss, increased allocation of fat by sebaceous glands of the skin (seborrhea). The mechanism of biotin action: as a coenzyme it is part of enzymes that increased the velocity of carboxylation reactions. Source of vitamin H are the liver and kidneys of cattle, eggs, milk, tomatoes, soybeans, carrots, potatoes, peas. The intake of biotin in the organism is also possible from microbial symbionts. Vitamin-like substances In addition to the two main groups of vitamins, we distinguish group of chemicals, part of which is synthesized in the organism, but it has vitamin properties. These include choline, lipoic acid, vitamin В15, para-aminobenzoic acid, carnitine, linoleic and linolenic acid, vitamin U, inositol and others. Antivitamins are compound similar in structure to vitamins, which compete with vitamins in the relevant biochemical processes or switch-off vitamins of the metabolic processes by means of their destruction or binding. An example of competing antivitamins is structural analogues of vitamin PP. They are able to form pseudo-coenzymes which simulate NAD+ and block the activity of NAD+-dependent oxidoreductases. An example of switch-off antivitamins is avidin – the protein of egg white, which forms insoluble biologically inactive complex with vitamin H. Since bacteria and viruses, as well as tumor cells have increased sensitivity to the lack of some vitamins, antivitamins are used as therapeutic agents. Test Questions 1. Give known classifications of vitamins. 2. Describe the biological role of vitamins. 3. Give the definitions of avitaminosis, hypovitaminosis, hypervitaminosis. 4. What are the causes of avitaminosis and hypovitaminosis of the human organism? 5. What substances are called antivitamins? How do they work? 6. List fat-soluble vitamins. Describe their biochemical functions. 7. List water-soluble vitamins. Derivatives of what vitamins are coenzymes, transferring methyl and amino groups? 8. Explain why the sulfonamide drugs cause death of the bacteria and can be used as medicine? 9. What vitamins can be used in the treatment of skin diseases? Phosphatidylcholine
2. Sphingolipids (sphingomyelins) - Lipids containing amino alcohol sphingosine.
3. Glycolipids - carbohydrate compounds in which the carbohydrate part of the covalently bound lipid. A characteristic feature of the molecules of phospholipids and glycolipids is their amphipathic charactere, one end of the molecule is hydrophobic and the other is hydrophilic. 4. Steroids are represented by cholesterol:
Proteins may be completely or partially embedded in the membrane ( intrinsic, or integral proteins and semi integral proteins ) or placed on its surface ( extrinsic, or peripheral proteins ). Sites of protein, which are turned into the extracellular medium, may be glycosylated. The protein composition of different membranes is different. Membrane proteins perform different functions: structural proteins, enzymes, proteins carrying out the transmembrane transport of metabolites, hormone receptors. Biological membranes are composed of a lipid bilayer of the small thickness (6 - 10 nm). The membranes are asymmetric in their original structure, which provides the gradient of the curvature and the spontaneous formation of closed structures. Typically, plasma membrane proteins are highly glycosylated from the extracellular medium. Intracellular membranes contain few glycoproteins and glycolipids and are characterized by lower microviscosity. Therefore, they can form small organelles. Cell membranes form significant limitations to the transfer of substances. The main obstacle is the hydrophobic region of the membrane. However, membranes are not impermeable structures. One of the main functions of membranes is regulation of substances transfer.
Fig. 15. The structure of the biological membrane
Facilitated diffusion Lipid bilayer is almost impermeable for larger polar molecules (glucose, amino acids), as well as for ions, as its interior is hydrophobic. These substances are transported across the membrane on the gradient of concentration, but with the participation of membrane proteins. 2a. Transfer through ion channels. Transmembrane transport of several ions (Са2+, Na+, K+, C1− ) occurs through ion channels. These are intrinsic proteins of membrane. They form a transmembrane hydrophilic (water-filled) channel. The selectivity of channels to ions is determined by the presence of specific center in protein canal for ion linking. Channels can be either closed or open. Signal to change the state of the channel may be a hormone or other signaling molecule. The example of controlled channels is Ca-channels. 2b. Transfer by transmembrane carrier protein (translocase). Each substance or group of similar substances has its own carrier. Transferred substance joins to the translocase. Then carrier changes its conformation. The substance is released from the other side of the membrane. Since there is no hydrophobic barrier, this mechanism is called facilitated diffusion. Example is facilitated diffusion (uniport) of glucose in erythrocytes with GLUT-1. Molecule of glucose links to translocase on the outer surface of the plasma membrane. Conformational change occurs, and the center of the carrier, occupied by glucose, is open inside the cell. As a result of conformational changes a carrier loses affinity for glucose, and the molecule is released in the cell cytosol. Separation of glucose causes a conformational change of the carrier protein, and it returns to the original conformation. Passive transport does not require energy.
Fig. 16. a - types of transport, b - passive and active transport: 1 - passive diffusion, 2 - diffusion through the channel, 3 - diffusion through the carrier, 4 - the active transport, 5 - secondary-active transport.
Active transport of substances occurs against the concentration gradient and it is associated with the supply of metabolic energy. In this way, there is transfer of many mineral ions from the extracellular fluid into the cell or in the opposite direction, the transfer of amino acids from the intestinal lumen into the cells of the intestine, transport of glucose from the primary urine through the kidney tubules cells in the blood. The main source of energy for active transport is ATP. Therefore, as a rule, these systems are ATPases. The example is Na+, K+-pump. There is an integral plasma membrane protein sodium-potassium ATPase. It moves potassium ions into the cell, and sodium ions from the cell. ATPase attaches inside of the membrane three Na+ ions. These ions alter the conformation of the active site of ATPase, and it hydrolyzes one molecule of ATP and attaches phosphate. The released energy is used to change the conformation of ATPase, after which three sodium ions are on the outer side of the membrane, and the phosphate ion is replaced by 2 K+ ions from the outside. Then, the carrier conformation changes to the original, and K+ ions are inside membrane. Here, K+ ions are split off, and the carrier is again ready for use. The work of Na+, K+-pump creates not only the difference in concentration, but difference in charges. On the outer side of the membrane a positive charge is created, and negative charge is inside. It is necessary for the nerve impulse transmittion. Secondary active transport. It is cotransport system. The gradient of a substance is used to transport the other. Carrier in this case has specific binding sites for both substances. The substance is transported against its concentration gradient by symport or antiport. Symport and antiport can occur due to the energy of the concentration gradient of Na+ ions, produced by Na+, K+-pump. In this way there is, for example, amino acid absorption from the intestine and the glucose from the primary urine and intestines. An example of secondary-active symport is transport of glucose and sodium ions, secondary-active antiport - Ca, Na-active transport. The secondary active transport has probably the greatest value for transfer of carbohydrates, amino acids and other metabolites in comparison with other mechanisms. There are special mechanisms for the transport of proteins, polysaccharides, and nucleic acids through the membrane. These are endocytosis (phagocytosis and pinocytosis) and exocytosis. Violation of the transport functions is due to more than 20 “ transport diseases ”, including renal glucosuria, cystinuria, malabsorption of glucose, galactose, and vitamin B12. Test Questions 1. List the basic cell membrane structures. 2. What is the qualitative and quantitative composition of membranes? 3. What lipids are parts of biological membranes? What are their properties and functions? 4. What is the difference between peripheral and integral proteins of biological membranes? 5. What factors can cause changes in the structure and permeability of the membrane? 6. List types of substances transport through the membrane. Which of them require an expenditure of energy? 7. What is the role of ATP-ase in the functioning of biological membranes?
TRANSMEMBRANE TRANSDUCTION OF THE HORMONAL SIGNAL Hormones are substances of organic nature, which are produced in the specialized cells of the endocrine glands, enter into the bloodstream and have a regulating effect on the metabolism and physiological functions. The specific characteristics of the biological action of hormones: hormones exert their biological effects in very small concentrations (from 10-6 to 10-12 M); the hormonal effect is realized through protein receptors and intracellular second messengers; hormones increase the rate of enzyme synthesis de novo or change the velosity of enzymatic catalysis; the hormones effect in the whole organism is determined to some extent by controlling influence of the CNS. Modern classification of hormones is based on their chemical nature. 1. Peptide and protein hormones include from 3 to 250 or more amino acid residues, for example, hormone of the hypothalamus and pituitary gland (growth hormone, corticotropin and others), and pancreatic hormones (insulin, glucagon). 2. Amino acid derivatives. These are adrenaline and thyroid hormones. Hormones of these two groups are highly soluble in water. 3. Steroid hormones. All of them are formed from cholesterol. These are corticosteroids, sex hormones (estrogens and androgens), hormonal form of vitamin D. Steroid hormones are lipophilic substances, easily penetrating the cell membrane. 4. Eicosanoids are hormone-like substances that have a local effect. They are derived from polyunsaturated fatty acid – arachidonic acid. Cell membranes due to the presence of specific receptors receive signals from the environment (for example, molecules of hormones, called primary messengers or intermediaries). The first stage of the hormone action on the target cell is its binding to the receptor, and then the signal is transmitted into the cell. By its chemical nature, almost all the receptors of biologically active substances are glycoproteins. A common property of all receptors is their high specificity towards one specific hormone. Adenylatecyclase messenger system is the most studied system(Fig. 17). It involves: 1) hormone receptor, and 2) the enzyme adenylyl cyclase, and 3) G- protein, and 4) cAMP -dependent protein kinase 5) phosphodiesterase.
The molecules of the protein hormones (insulin), hydrophilic molecules (adrenaline) cannot pass through the cell membrane. Their receptors are located on the membrane. Binding of hormone ( the primary messenger ) to the receptor leads to structural changes in the receptor intracellular domain. It provides interaction of the receptor with GTP-binding protein (G-protein). G-protein is a mixture of two types of proteins: active Gs (from the Eng. stimulatory) and inhibitory Gi. They have three different subunits (α, β and γ ). The function of G-protein is carrying out a hormonal signal at the plasma membrane. Hormone-receptor complex transforms Gs-protein in the activated state. It is activated by dissotiation of G-protein subunits. The active G-protein activates adenylate cyclase. Adenylate cyclase is almost inactive in the absence of G-protein. Adenylate cyclase is an integral plasma membrane protein and its active site is oriented toward the cytoplasm. Adenylate cyclase catalyzes the reaction of synthesis of cAMP from ATP. cAMP is a second messenger. Under the action of cAMP inactive protein kinase turnes into active form. This enzyme catalyzes the phosphorylation of intracellular enzymes or target proteins, changing their activity. This reaction goes with the participation of serine, threonine, tyrosine OH-groups. Phosphorylation and dephosphorylation of proteins with the participation of protein kinases is a common fundamental mechanism of secondary messengers within the cell. Phosphodiesterase causes the breakdown of cAMP and thereby terminates the hormonal signal.
Steroid and thyroid hormones are lipophilic and can easily pass through cell membranes. The receptors of these substances are in the cytosol or nucleus of the cell ( intracellular receptors ). Complex of hormone with a receptor is formed in the cytosol, and then enters the nucleus. Hormone-receptor complex passes into the nucleus and interacts with a regulatory nucleotide sequence in DNA. Accordingly, the rate of transcription of structural genes and the rate of translation are changed. Consequently, the amount of proteins, which may affect the metabolism and functional state of the cell, is also changed (Fig. 18).
Complex " hormone - receptor" may be formed directly in the nucleus. Thyroid hormone receptors are always associated with DNA. Hormones provide a communication (information exchange) between different cells and organs. As a result of these mechanisms, coordination of metabolism and functions of different cells and organs and adequate reaction to changes in the environment are achieved. The role of extracellular signals not only hormones can performe, but also a number of other substances - cytokines, biogenic amines, neurotransmitters, etc. Test Questions 1. What is the transmembrane transfer of signals? 2. Which compounds can act as primary messengers, second messengers? 3. Describe the main parts and the mechanism of action of adenylatecyclase messenger system. 4. List the major types of regulation of enzyme activity in the cell.
6. INTRODUCTION TO METABOLISM Metabolism (from the Greek " transformation, change" ) is a set of chemical reactions in living cells, providing growth, development and activity of the body and life in general. Metabolism consists of two opposing simultaneous processes. Catabolism includes reactions associated with the breakdown of substances, their oxidation and elimination of waste products from the body. Catabolic reactions are exergonic (give energy). The organelles of catabolic system are mitochondria, lysosomes, peroxisomes. (Peroxisomes are cellular organelles, which are carrying out the oxidation of fatty acids, the synthesis of bile acids, cholesterol, etc. Glioxysomes are a kind of peroxisomes, in which the oxidation of glyoxylate cycle and the Krebs cycle going on.) Anabolism integrates all reactions associated with the synthesis of essential substances, their assimilation and use for growth, development and functioning of the body. Anabolic reactions are usually endergonic (energy consuming). The organelles of anabolic system are endoplasmic reticulum and ribosomes, Golgi apparatus. Metabolites are products of metabolism of some compounds. Stages of metabolism: 1. Intake of substances in the body (breathing, eating, digestion). By digestion polymers (starch, proteins, fats) break down to monomers (amino acids, glucose, etc.), which pass into the blood. 2. Intracellular metabolism (intermediate exchange) is a set of metabolic pathways. Metabolic pathways are the consistent transformation of one substance into another, of one metabolite into another. There is usually a reaction in the pathway with a slower rate than others. It is the rate-limiting stage ( reaction ). It determines the overall rate of conversion of a substance into a final product of the metabolic chain. The enzyme that catalyzes the rate-limiting reaction is called regulatory one. The reactions of metabolism are mainly reversible. Their direction is determined by consumption or removing of the product. Under constant conditions, the concentration of several metabolites in cells and extracellular fluids is constant. In diseases, the steady-state concentrations of metabolites are specifically changed. It is the base of biochemical methods of laboratory diagnostics of diseases.
6.1. STAGES OF CATABOLISM Stages of catabolism I. Hydrolytic stage. Proteins, fats and carbohydrates are broken down into the corresponding monomers under the influence of hydrolases in the digestive tract. II. Specific pathways of catabolism. Monomers of major nutrients (with the participation of enzymes that are specific to each class of substances) are transformed into two metabolites - pyruvic acid and acetyl-CoA. At this stage, 1/3 energy of nutrients is released. Acetyl-CoA (acetyl coenzyme A) is the energy-rich product of condensation of coenzyme A with acetic acid. It includes pantothenic acid. Coenzyme A is in the free state in the cell and interacts with the enzyme at the moment of reaction with the substrate. Carbohydrate METABOLISM Digestion of carbohydrates Carbohydrates of foods are carbohydrate source of the organism. Usage rate is 400-500 grams per day. Carbohydrates are the major source of energy needed to man. Carbohydrates as a part of glycoproteins also performe protective function. They are used for synthesis of NA. Starch is accumulated in plants, lactose is present in breast milk, glucose and fructose are in honey and fruits, and maltose comes from the foods in which starch is partially hydrolyzed, such as malt. Annual consumption of carbohydrates is 400-500 g/day, with them comes the principal amount of calories needed to man. Food poly- and disaccharides undergo enzymatic digestion in the digestive tract, where the enzymatic hydrolysis of glycosidic bonds goes. Monosaccharides are formed, then they are absorbed, enter the blood and tissues. a-amylase of saliva decomposes a-1, 4-glycosidic bonds. Starch is partially digested in the mouth. Dextrins and maltose are formed. Gastric juice does not contain enzymes that break down dietary carbohydrates. Saliva amylase is inactivated in the stomach, because pH of gastric juice is 2, and pH optimum of amylase of saliva is 6.7. But amylase acts any time inside the food bolus. Pancreatic amylase hydrolyzes starch in the upper small intestine by sequential cleavage of disaccharide residues. Maltose and isomaltose are formed. Maltose, isomaltose, sucrose, lactose are hydrolyzed by glycosidases on the cell surface of the small intestine to monomers (maltose is hydrolyzed by the enzyme maltase to glucose, sucrose is hydrolyzed by the enzyme sucrase to glucose and fructose). b-Cellulose is not cleaved in the gastrointestinal tract: a person cannot produce an enzyme hydrolyzing 1, 4-glycoside bonds. Undigested cellulose of plant foods promotes normal bowel movements. Glucose transport across the membrane occurs by facilitated diffusion or active transport. Na+-glucose co-transporter, or simporter, carries the secondary active transport of glucose. Concentration gradient of Na+ is maintained through the work of Na+, K+-pump. Galactose is transported by the same way. Glucose can be transported across the membrane also by facilitated diffusion with the help of carrier proteins. There are five types of glucose transporters (GLUT).The rate of the transmembrane transport of glucose depends on its concentration gradient. Exceptions are muscle cells and adipose tissue, where there are insulin-dependent transporters. In the absence of insulin, the membrane is impermeable to glucose. Fructose is also absorbed by facilitated diffusion. Hereditary or acquired defects of enzymes that hydrolyze carbohydrates is one of the causes of digestive disorders. The accumulation of undigested carbohydrates increases the flow of water into the lumen of the intestine that causes spasms and diarrhea. The action of bacteria on non-hydrolyzed carbohydrates leads to flatulence. Most of the glucose (90%) comes from the blood through the portal vein to the liver. In the cell, glucose is phosphorylated (the active form) and subjected to further transformations.
GLYCOGEN METABOLISM Glycogen is the main reserve homopolysaccharide of a human. A monomer of glycogen is glucose. Glucose residues are connected in linear chains by 1, 4-a-glycoside bonds. Branches are formed by1, 6-a-glycoside bonds. The branched structure of glycogen causes many terminal monomers. It is important for enzymes working at glycogen decay or synthesis. Glycogen is deposited in the liver and skeletal muscle and stored in the cytosol in the form of pellets. Metabolic pathways of glycogen synthesis and degradation are different. Glycogen synthesis (glycogenesis) occurs within 1-2 hours after intake of carbohydrate foods and requires consumption of ATP. This process reduces the glucose level in the blood. 1). Phosphorylation of glucose with the participation of hexokinase (in muscle) and glucokinase (in liver) gives glucose-6-phosphate, which transforms into glucose-1-phosphate (enzyme is phosphoglukomutase): 2). Glucose-1-phosphate reacts with UTP with the participation of glucose-1-phosphate uridil transferase. UDP-glucose and pyrophosphate are formed: 3). Transfer of glucose residue from UDP-glucose to a small fragment of pre-existing glycogen chain (“primer”) goes under the action of glycogen synthase: UDP-G + glycogen (n) ® UDP + glycogen (n+ 1) Glycogen synthase catalyzes the formation of a-1, 4-glycosidic bonds. In the absence of glycogen a specific protein glycogenin can accept glucose from UDP-glucose. Glycogen branching enzyme (glucosyl α -4, 6 transferase) provides formation of 1, 6-α glycosidic bonds. It transfers the oligosaccharide fragments (6-7 glucose residues) to the 6-hydroxyl group of glucose residue of the same or different chains of glycogen where it is linked by α -1, 6-bond. The degradation of glycogen (glycogenolysis) is a conversion of glycogen from reserve form in the metabolic form (glucose). In the presence of phosphorylase glycogen is degraded into glucose-1-phosphate without splitting on fragments. Glycogen phosphorylase exists in two forms - phosphorylase a (active) and phosphorylase b (inactive). Both forms can dissociate into subunits. Phosphorylase b consists of two subunits, phosphorylase a consists of 4 subunits. The conversion of phosphorylase a into phosphorylase b is accomplished by phosphorylation of protein under the action of phosphorylase kinase: 2 Phosphorylase b + 4 ATP → phosphorylase a + 4 ADP. Inactive phosphorylase kinase becomes active under the influence of the enzyme cAMP-dependent protein kinase. cAMP is formed from ATP under the action of adenylate cyclase that is activated by adrenalin and glucagon. As a result, glycogen breaks down and forms glucose-1-phosphate. A limit dextrin is formed, which is cleaved under the action of a bifunctional enzyme (debranching enzyme). It has transferase activity and α -1, 6-glucosidase activity and releases a free glucose. Then glycogen again can be degraded by phosphorylase. Glucose-1-phosphate under the influence of phosphoglucomutase is converted into glucose 6-phosphate. Glucose is formed in the liver from glucose-6-phosphate by hydrolytic cleavage of phosphate (enzyme is glucose-6-phosphatase). G-1-P ® G-6-P ® G
GLYCOLYSIS Glycolysis (Embden – Meyerhof pathway) is the sequence of enzymatic reactions that lead to the splitting of glucose with the formation of pyruvic acid or lactate, accompanied by the formation of ATP. This process occurs in the cell cytosol. In aerobic glycolysis pyruvate is formed. It enters the mitochondria, and further, in the common catabolic pathway, is oxidized to CO2 and H2O. Aerobic glycolysis is the part of aerobic degradation of glucose. In anaerobic glycolysis pyruvate is formed and then is converted to lactate. Anaerobic degradation of glucose and anaerobic glycolysis are synonyms. Anaerobic glycolysis occurs in the first few minutes of muscular work, in erythrocytes (there are no mitochondria in erythrocytes), and when there is insufficient intake of oxygen. Reactions of glycolysis: 1). Phosphorylation of glucose. The reaction is catalyzed by hexokinase, in parenchymal liver cells it is catalyzed by glucokinase. The formation of glucose-6-phosphate in the cell is a trap for glucose, because membrane is impermeable for phosphorylated glucose. It is irreversible reaction. Hexokinase has low Km, glucokinase has high Km.
2). Isomerization reaction is catalyzed by glucose-6-phosphate isomerase (phosphoglucose isomerase):
3) Phosphorylation reaction is catalyzed by 6-phosphofructokinase. This is irreversible and the rate-limiting reaction.
These three reactions are reactions of energy investment phase. 4). Aldol splitting reaction is catalyzed by aldolase.
5). Isomerization of dihydroxyacetonephosphate is catalyzed by enzyme triosephosphate isomerase:
1 molecule of glucose is converted to 2 molecules of glyceraldehyde-3-phosphate (reactions 4, 5). This was splitting phase. The next stage is energy generation phase. 6). The oxidation of glyceraldehyde-3-phosphate goes under the action of enzyme glyceraldehyde-3-phosphate dehydrogenase:
7). Substrate level phosphorylation goes on with the participation of phosphoglycerate kinase:
8). Intramolecular transfer of a phosphate group. The enzyme is phosphoglycerate mutase:
9). Dehydration with the participation of enolase:
10). Substrate level phosphorylation. The enzyme is pyruvate kinase:
This is irrevesible reaction. 11). Under anaerobic conditions, the reduction of pyruvate to lactate occurs. Reaction is catalyzed by lactate dehydrogenase:
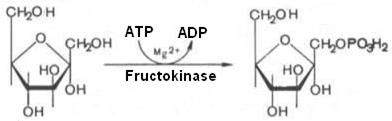
The overall equation of anaerobic glycolysis: glucose + 2 NAD+ + 2 ADP + 2 Pi ® 2 pyruvate + 2 NADH + 2 ATP Anaerobic glycolysis does not require the mitochondrial respiratory chain. The yield of ATP from anaerobic glycolysis: ATP is formed in two reactions of substrate level phosphorylation. 4 ATP molecules are formed by 1 glucose molecule (1 glucose molecule gives 2 trioses, and each gives 2 ATP in 7th and 10th reactions of glycolysis.). 2 ATP are consumed (reaction 1 and 3 of glycolysis) and 4 ATP - 2 ATP = 2 ATP. The yield of ATP in aerobic degradation of glucose: - three reactions of substrate level phosphorylation (7th, 10th - glycolysis; 5th – Krebs cycle) = 3ATP; - five reactions of dehydrogenation with the formation of NADH (6th - glycolysis, 3rd - oxidative decarboxylation of pyruvate; 3rd, 4th, 8th - Krebs cycle) Þ 3x5 = 15ATP; - dehydrogenation reaction (6th - Krebs cycle) with the formation of FADH2 = 2 ATP; total: 3ATP + 15 ATP + 2ATP= 20 ATP. From 1 molecule of glucose 2 molecules of glyceraldehydes-3-phosphate are produced, then 2 х 20ATP = 40 ATP. In reactions 1 and 3 of glycolysis 2ATP are consumed, and 40ATP - 2ATP = 38ATP. In glycolysis The inclusion of fructose in metabolism in the liver begins with phosphorylation reaction catalyzed by the formation of fructose-1-phosphate:
Fructose-1-phosphate is split by aldolase on glyceraldehyde and dihydroxyacetone phosphate. Dihydroxyacetone phosphate is included in the fifth reaction of glycolysis. Glyceraldehyde may be included in glycolysis after its phosphorylation with ATP. The resulting glyceraldehyde-3-phosphate is included in the sixth reaction of glycolysis. Fructose metabolism in muscle, kidney, and adipose tissue begins with its phosphorylation by hexokinase and ATP involvement. Fructose-6-phosphate is formed. The reaction is inhibited by glucose. Next, fructose-6-phosphate is converted to fructose-1, 6-bisphosphate and is included in the fourth reaction of glycolysis. Galactose is produced in the intestine by hydrolysis of lactose. To convert galactose into glucose, it is necessary to carry out the reaction of epimerization. This reaction in the cell is only possible with uridine diphosphate-derivative of galactose (UDP-galactose). Initially, galactose is phosphorylated. Galactose-1-phosphate is formed. Then: Gal-1-P + UDP-G « G-1-P + UDP-Gal, enzyme is hexoso-1-phosphate uridyltransferase. UDP-galactose undergoes epimerisation: UDP-Gal « UDP-G, enzyme is UDP-hexose-4-epimerase. UDP-G + PPi « G-1-P + UTP, enzyme is UDP-glucose-pyrophosphorilase. G-1-P under the action of phosphoglucomutase is converted into G-6-P and then is included in the second reaction of glycolysis as usual, or G-1-P under the action of phosphatase is converted to glucose. THE SHUTTLE MECHANISMS Cytosolic NADH (glycolysis reaction 6) cannot transfer hydrogen to the respiratory chain, because the mitochondrial membrane is impermeable to it. Transport of hydrogen through the membrane occurs with the help of special systems, called " shuttle". Hydrogen is transported through the membrane with the participation of pairs of substrates. On both sides of the mitochondrial membrane there is a specific dehydrogenase. Glycerol-phosphate shuttle system operates in cells of the white muscle, liver and brain. Hydrogen from NADH in the cytosol is transferred to dihydroxyacetone phosphate by glycerol-3-phosphate dehydrogenase (NAD-dependent enzyme). The resulting glycerol-3-phosphate is oxidized by the enzyme of mitochondrial inner membrane glycerol-3-phosphate dehydrogenase (FAD-dependent enzyme). Then, protons and electrons from FADH2 pass to ubiquinone, and further along the respiratory chain.

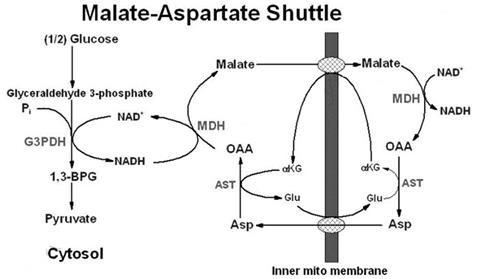
1 – glyceraldehyde-3-phosphate dehydrogenase; 2 - glycerol-3-phosphatede hydrogenase (cytosolic enzyme); 3 - glycerol-3-phosphate dehydrogenase (mitochondrial enzyme). Malate-aspartate shuttle system includes malate, cytosolic and mitochondrial malate dehydrogenase. This system is more universal, and works in the cardiac muscle, liver and kidneys. In the cytoplasm NADH reduses oxaloacetate to malate. Malate is transported across mitochondrial membrane with the carrier help. In matrix malate is oxidized to oxaloacetate by NAD-dependent malate dehydrogenase. Redused NADH gives hydrogen to the mitochondrial respiratory chain.
Oxaloacetate formed from malate cannot go from mitochondria to the cytosol: membrane of mitochondria is impermeable to it. Therefore, oxaloacetate is converted to aspartate, which is transported into the cytosol, where it again turns into oxaloacetate. Both shuttle systems differ by the number of synthesized ATP. In the first system 2 ATP are formed (hydrogen is introduced into the respiratory chain at the level of ubiquinone). The second system is more energy efficient. It gives 3ATP (hydrogen enters the respiratory chain with the mitochondrial NAD+). CORI CYCLE Cori cycle (glucose-lactate cycle) has opened a Czech scientist and Nobel Prize winner Theresa Cori. During intense muscular work and in the absence or insufficient number of mitochondria (e.g., in erythrocytes) glucose undergoes anaerobic glycolysis with lactate formation. When there is the accumulation of lactate in the muscles lactic-acidosis occurs. Sensory nerve endings are irritated, causing pain in the muscles.
Lactate is transferred by blood to the liver and is converted to pyruvate and then into glucose. Glucose synthesis is gluconeogenesis. Then glucose with the blood flow can return to the working muscle. Direction of lactate dehydrogenase reaction in the working muscles and the liver determined by the concentration ratio of reduced and oxidized forms of NAD+: ratio of NAD+ / NADH in contracting muscle is more than in liver.
ALCOHOLIC FERMENTATION Alcoholic fermentation is carried out by yeast organisms, as well as some of the mold:
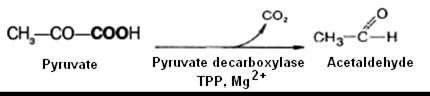
The reaction mechanism is similar to glycolysis. The divergence starts after the stage of pyruvate formation. During glycolysis pyruvate is reduced to lactate by the enzyme LDH (lactate dehydrogenase) and the coenzyme NADH. During alcoholic fermentation pyruvate undergoes decarboxylation, acetaldehyde is formed as a result, and then during its reduction ethanol is formed:
During lactic acid fermentation pyruvate is not decarboxylated, and, as in glycolysis in animal tissues, it is redused with the participation of LDH due to the hydrogen of NADH. C6H12O6 → 2 CH3CHOHCOOH PENTOSE PHOSPHATE PATHWAY (HEXOSE MONOPHOSPHATE SHUNT) Pentose phosphate pathway is an alternative way of glucose oxidation. Its functions are: - to supply to cells coenzyme NADPH, used as a hydrogen donor in biosynthetic reactions; - to provide cells with pentose phosphates for the synthesis of nucleotides and nucleic acids. Pentose phosphate pathway does not lead to the synthesis of ATP. Pentose phosphate pathway of pentose formation occurs in the liver, adipose tissue, lactating mammary gland, tests, adrenal cortex, erythrocytes. The enzymes of pentose phosphate pathway are located in the cytosol. In the pentose phosphate pathway of glucose conversion oxidative and non- oxidative pathways are released. Oxidative phase includes two reactions of dehydrogenation. Coenzyme of dehydrogenase is NADP+. Pentoses are formed by oxidative decarboxylation. 1. Dehydrogenation of glucose-6-phosphate with the participation of glucose-6-phosphate dehydrogenase and coenzyme NADP+ gives 6-phosphoglucono-d-lactone and NADPH:
The 1st reaction is the most regulatory in the HMP shunt. NADPH is an inhibitor of glucose-6-phosphate dehydrogenase. 2. 6-Phosphogluconolactone is unstable and is hydrolyzed to 6-phosphogluconate under the action of 6-phosphoglucono lactonase:
3. Dehydrogenation and decarboxylation of 6-phosphogluconate to form ribulose-5-phosphate (pentose) and NADPH with the participation of decarboxylating 6-phospho-gluconate dehydrogenase:
4. Xyluloso-5-phosphate (pentose) is formed from ribulose-5-phosphate under the action of epimerase. Under the influence of ketoisomerase ribulose-5-phosphate is converted to ribose-5-phosphate (pentose). Between the forms of pentose phosphates equilibrium is established:
At this stage, the pentose phosphate pathway can be completed. Under anaerobic conditions, there a non-oxidative stage of pentose phosphate cycle comes. Non-oxidative stage includes reactions of transfer of 2 - and 3-carbon fragments from one molecule to another. The process is reversible, and hexoses can be formed from pentoses. Intermediates of glycolysis are formed (fructose-6-phosphate, fructose-1, 6-bisphosphate, phosphotrioses), and substances that are specific to the pentose phosphate pathway (sedoheptulose-7-phosphate, pentose-5-phosphate, erythrose-4-phosphate). Six molecules of glucose-6-phosphate in the pentose phosphate cycle form 6 molecules of ribulose-5-phosphate and 6 molecules of CO2. CO2 is formed from C-1 carbon atoms of six molecules of glucose-6-phosphate. Then 5 molecules of glucose-6-phosphate are regenerated by 6 molecules of ribulose-5-phosphate. The overall equation: 6 Glucose 6-phosphate + 12 NADP+ + 7 H2O ® ® 5 Glucose 6-phosphate + 12 NADPH + 12H+ + 6 CO2 The intermediates of the cycle (fructose-6-phosphate and glyceraldehyde 3-phosphate) are included in glycolysis. Gluconeogenesis Gluconeogenesis is a glucose synthesis from substances of non-carbohydrate nature, which takes place mainly in the liver, and less intense - in the cortex of kidney and intestinal mucosa. The function of gluconeogenesis is the maintenance of blood glucose during prolonged fasting and intense exercises. A constant supply of glucose as an energy source is particularly necessary for the nervous tissue and erythrocytes. Gluconeogenesis substrates are pyruvic acid, lactic acid, glycerol, amino acids. Their inclusion in gluconeogenesis depends on the physiological state of the organism. Most of the reactions of gluconeogenesis are the inverse of glycolysis. They are catalyzed by the same enzymes as the corresponding reactions of glycolysis. Three reactions of glycolysis (hexokinase (1), phosphofructokinase (3), pyruvate kinase (10)) are irreversible, and during gluconeogenesis other enzymes operate on these stages.
Glycogenosis Glycogenosis is a group of inherited diseases caused by deficiency of enzymes involved in synthesis or breakdown of glycogen. Glycogenosis of 0 type occurs under glycogen synthase deficiency. It is characterized by a sharp decrease of glycogen in the liver, there is a condition until the development of coma (hypoglycemic syndrome). Patients with glycogen synthase deficiency die at an early age. Lack of enzymes involved in the breakdown of glycogenleads to its accumulation in organs and tissues (Table 1). Table 1. The diseases associated with metabolic disorders of glycogen.
Hyper- and hypoglycemia Under some conditions increase of glucose in blood can be observed. It is called hyperglycemia, and lowering the concentration of glucose is called hypoglycemia. Changes of glucose levels over time in blood are investigated for the diagnosis of hyperglycemia, usually after taking 50 grams or 100 grams of glucose dissolved in warm water. It is the so-called sugar load – glucose tolerance test. Blood and urine samples are collected every 30 minute. When assessing the glycemic curves we pay attention to the time of maximum lifting, height of the rise and time for the glucose concentration to return to the original level.
In a healthy person after taking the glucose its amount in the blood is increased, reaching the peak after 30-45 minutes. Then its concentration in the blood begins to decrease and after 2 hours reduces to normal, but after 3 hours it is even slightly below normal (Fig. 22). There is a number of indicators to evaluate the glycemic curves, the most important factor of which is a coefficient of Baudouin: [(В-А)/А]х100, %, where A – is the level of glucose in blood in an empty stomach; B – is the maximum glucose in blood after glucose load. Normally, this ratio seems to be about 50%. Values exceeding 80% indicate a serious disorder of carbohydrate metabolism. Hormonal hyperglycemia occurs in any disturbance of the function of endocrine glands, hormones of which are involved in the regulation of carbohydrate metabolism. One of the hyperglycemia’s reasons is diabetes mellitus. Type 1 diabetes (insulin-dependent diabetes mellitus, IDDM) is associated with decreased formation of insulin. Usually it begins in childhood (12-15 years of age) as a consequence of autoimmune destruction of β -cells in the islets of the pancreas. Type 2 diabetes begins in adulthood, develops gradually. Mechanisms of insulin signal transduction are damaged; the concentration of insulin in the blood may be normal or even elevated (insulin-independent diabetes mellitus, NIDDM). Receptors of target cells lose the ability to connect with a molecule of insulin. Carbohydrate metabolism in diabetes mellitus is characterized by: 1. Glucokinase and glycogen syntase synthesis is sharply reduced, resulting in a sharp slowdown in the synthesis of glycogen. 2. Activity of glucose-6-phosphatase increases sharply, so the glucose-6-phosphate is dephosphorylated and enters the blood in the form of glucose. 3. Transport of glucose across cell membranes is reduced. 4. Gluconeogenesis is accelerated because insulin suppresses the activity of pyruvate carboxylase and glucose-6-phosphatase. Thus, excess production and lack of use of glucose tissue occur in diabetes mellitus, causing hyperglycemia. Glucose in blood in severe forms can be up to 4-5 g/l and above. A body's homeostatic mechanism, when operating normally, restores the blood sugar level to a narrow range of about 4.4 to 6.1 mmole/l (0, 82 to 1, 10 g/l). The osmotic pressure of the blood is increased, which leads to dehydration of body cells. In connection with dehydration functions of the central nervous system are disturbed (hyperosmolar coma). Glycemic curve ( Glycemic index graph ) in diabetes compared with that in healthy people is considerably stretched in time (Fig. 22). Hyperglycemia is also being developed with an increase in production of glucagon - the hormone of α -cells of islets of Langerhans of the pancreas, which activates phosphorylase of the liver and promotes glycogenolysis. Similar action is typical of adrenaline. An excess of glucocorticoids leads to hyperglycemia (which stimulates gluconeogenesis and inhibits hexokinase) and pituitary growth hormone (inhibits the synthesis of glycogen, promotes the formation of an inhibitor of hexokinase). Hyperglycemia sometimes occurs during pregnancy, organic lesions of the central nervous system, liver disease of inflammation or degenerative nature. Hypoglycemia is associated with a decrease in function of those endocrine glands, increasedfunctions of which lead to hyperglycemia. Hypoglycemia can be observed at Addison's disease (Addison’s disease is a chronic endocrine disorder - adrenal insufficiency, hypocortisolism, and hypoadrenalism), hypothyroidism, adenoma of the pancreas due to increased production of insulin. Hypoglycemia can be caused by starvation, prolonged physical work, taking β -ganglioplegics, sometimes it is observed during pregnancy and lactation. Hypoglycemia may occur when high doses of insulin are administered to patients with diabetes mellitus. Glycosuria Glycosuria is the result of altered carbohydrate metabolism as a result of pathological changes in the pancreas (diabetes mellitus, acute pancreatitis, etc.). In severe forms of diabetes glucose in the urine can reach 8-10%. The osmotic pressure of urine is increased. The daily diuresis rises to 5-10 liters or more (polyuria). Dehydration develops as a consequence of it and increased thirst develops (polydipsia). Less frequent glucosuria of renal origin, associated with failure of resorption of glucose in the kidney tubules. Glycosuria may occur as a temporary phenomenon in some acute infectious and nervous diseases, after epilepsy, concussion. Poisonings by morphine, strychnine, chloroform, phosphorus, are usually accompanied by glucosuria. Glycosuria may be of nutritional origin, pregnancy glucosuria, and glucosuria with nervous stress states (emotional glycosuria). Fructosuria is congenital deficiency of the enzyme fructokinase (fructose-1-phosphate is not formed). The accumulation of fructose in blood leads to fructosuria. Galactosemia. The reason is lack of the enzyme hexose-1-phosphaturidil transferase. It is characterized by accumulation of galactose and galactose-1-phosphate in the blood, vental retardation, cataracts of the lens.
Quiz Questions 1. List the major food sources of carbohydrates. What is the daily requirement for carbohydrates in the adult? 2. Describe the process of digestion and absorption of carbohydrates in the digestive tract. 3. Give the scheme glycogen synthesis from glucose, list the enzymes involved in this process. 4. Consider the mechanism of phosphorolytic cleavage of glycogen. What is the role of glycogen in the maintenance of glucose homeostasis? 5. What are the basic steps of glycolysis? What are the similarities and differences between aerobic and anaerobic glycolysis? 6. What is the energy value of breakdown of glucose under aerobic conditions? 7. What reaction includes measles cycle? What is its biochemical function? 8. What are the similarities and differences between glycolysis and fermentation? 9. What is meant by gluconeogenesis? What are the main stages of this process? 10. How does the glycerol phosphate shuttle mechanism and malate-aspartate shuttle system? 11. What is special about the exchange of fructose and galactose? 12. What are the hormones involved in regulating glucose homeostasis? 13. What is the chemistry of the pentose phosphate pathway of glucose metabolism? 14. What is the biological role of forming reduced forms of NADP? 15. List the disorders of carbohydrate metabolism that are known to you. 16. In what may be the cause of hyperglycemia and hypoglycemia?
II. LABORATORY PRACTICE
Millon’s reaction. Millon's reagent consists of nitrate of mercury (I) and (II) in HNO3 with admixture of HNO2. The reaction of Millon's reagent with protein due to the presence of tyrosine residue in them. In the test tube 0.5 ml protein solution is poured and 0.5 ml of Millon's reagent. A white precipitate is formed under the action of mercury salts and nitric acid, which are the part of Millon's reagent. When heated, the precipitate is colored in pink at first, and then in a brown-red color.
Ninhydrin’s reaction. The reaction is due to the presence of α -amino acids residues in the protein. 1 ml protein solution is poured in the test tube, 5 drops of 0.2% ninhydrin solution is added and heated. After a few minutes we observe the appearance of a blue-violet color.
+ R - СОН + СО2 + N Н3
Test questions 1. How can you separate the mixture of amino acids in the hydrolyzate of the protein? 2. What color reactions for proteins are known to you from the course of bioorganic chemistry? 3. Which amino acid is founded in proteins with the help of Millon’s reaction? Give its formula. 4. Which amino acid is in proteins, and founds during Adamkevich’s and Schulze – Raspel’s reactions? Give its formula. 5. What caused precipitation of proteins by the action of salts of heavy metals? 6. What is meant by denaturation of protein? 7. What is the practical application of the reaction of precipitation of proteins by organic acids? 8. Why in clinical practice for the protein precipitation using nitrogen rather than sulfuric or hydrochloric acid? Phosphoproteins. A typical representative of phosphoproteins is the casein of milk. Casein is decomposes into protein and phosphoric acid during the alkaline hydrolysis. Glycoproteins. Gastrointestinal mucins are glycoproteins, the carbohydrate part of which is represented by mucopolysaccharides. They protect mucous membranes from chemical, mechanical and thermal stresses and digestion by proteolytic enzymes. Test questions 1. Which proteins are called conjugated? 2. How does a bond between the polypeptide chain and phosphoric acid in phosphoprotein form? 3. Why do a special role for the fetus, embryo, and newborn phosphoproteins play? 4. What is the difference between glycoproteins and proteoglycans? 5. What types of relationships exist between the carbohydrate and protein components? 6. Why glycoproteins are less sensitive to the denaturation factors than simple proteins?
Nucleoproteins Deoxyribonucleoproteins (DNP) are isolated from tissues rich in cell nuclei (thymus, spleen, and sperm). DNP are dissolved in an average concentration of salts, such as sodium chloride (1 M), and again precipitated at a dilution of the latter (up to 0.15 M) in the form of fibrous nucleoprotein. Chromoproteins. The representative of chromoproteins is a protein of mammals erythrocytes - hemoglobin. Its protein part is globin and non-protein is heme (protoporphyrin, the pyrrole rings of which are linked to an iron atom). Test questions 1. List the functions of chromoproteins in the body. 2. Specify the structure of the protein part of hemoglobin. 3. Why the hemoglobin of the embryo and the child has a different affinity for oxygen? 4. After the fire dead was founded. How in a simple way we can to determine whether a person was killed in a fire or died before the fire? 5. Describe the chemical composition of nucleoproteins and their functions in the body. 6. What is more soluble in water: the nucleic acids or nucleoproteins? Why?
Laboratory work 4. Enzymes Test questions 1. What is the role of enzymes in an organism? 2. What class of chemical compounds do enzymes belong to? 3. What class do the enzymes used in the laboratory work belong to? 4. Why does inactivation of the enzymes solutions take place while boiling them? 5. How can you explain the specificity of sucrase and amylase enzymes? How can it be proved? 6. How does the lowering of pH influence the activity of α -amylase? Why? 7. On what principle is the qualitative definition of enzymes based on?
Test questions 1. What are activators and inhibitors of enzymes? 2. How can the influence of activators and inhibitors upon the work of enzymes be investigated? 3. The enzyme acetylcholinesterase catalyses the hydrolysis of acetylcholine. It is neuromediator produced in the synapses of cholinergic nerves. Its breakdown products - acetate and choline – are unable to work as neuromediators. The hydrolysis of acetylcholine is stopped by calimine – a medicinal preparation used to heal motor disturbance after injuries, paralysis, in rehabilitating periods after having poliomyelitis, encephalitis, etc. The following scheme reflects the inhibition of acetylcholinesterase: Inhibitor calimine
acetylcholine choline acetic acid
Compare the structural formulas of the inhibitor and the substrate. Why can one suppose that the inhibitor is bounding in the active centre of the enzyme? How will the influence of calimine change the conduction of nerve impulse (increase, reduce or will not change)?
Laboratory work 6. Vitamins Reaction with aniline. Pour 0, 5 ml of fish liver oil and 0, 5 ml of aniline and strong sulfuric acid mixture into a dry test tube (15: 1), mix properly, heat carefully up to boiling for a minute. If vitamin D is present, the color of this emulsion will be green and then - red. Leave the test tube at the room temperature. The emulsion is layered; the lower layer is turning bright-red.
Vitamin D (calciferol) Test questions 1. What substanses belong to vitamins? What is their general function in an organism? 2. List the biochemical functions of the vitamins which were identified in the laboratory work. 3. Define the terms: avitaminosis, hypovitaminosis and hypervitaminosis.
Test questions 1. What reactions catalyze the enzymes of oxidoreductases class? 2. Consider the role of dehydrogenases in the processes of biological oxidation. 3. For experiment 1 make up a scheme of hydrogen transfer (electrons and ions of hydrogen) taking into account standard oxidation-reduction potentials of the used components.
Test questions 1. What are the optimal conditions for pancreatic amylase functioning? 2. How can the presence of starch conversion products be identified in a test? 3. What classes do the enzymes, splitting glycogen into glucose, belong to? 4. What compounds are the products of aerobic and anaerobic glycolysis? 5. Why does the energetically wasteful anaerobic glycolysis remain in the organism? 6. What functional group of glucose molecule causes Trommer’s positive test? 7. What diseases or physical conditions cause glucosuria? 8. Name the reasons for fructosuria development. 9. How can sugar decrease in blood be explained after insulin injection?
References 1. Berezov, Т.Т. Biological chemistry. / Т.Т. Berezov, B.Ph. Korovkin. - М.: Open joint-stock society " " Medicine" publishing office", 2007. - 704 p. 2. Biochemistry. / Edited by Y.S. Severin. - М.: ГЭОТАР -Меdia, 2003. - 779 p. 3. Biochemistry. The short course with exercises and tasks. / Edited byY.S. Severin, А.Y. Nikolayev. - М.: ГЭОТАР - Меdia, 2001. - 448 p. 4. Zubairov, D.М. Study guide for laboratory works on biological chemistry. / D.M. Zuibarov, V.N. Timerbayev, V.S. Davydov. - М.: ГЭОТАР -Меdia, 2005. - 392 p. 5. Kushmanova, O.B. Study guide for laboratory works on biological chemistry. / О.B. Kushmanova, G.I. Ivchenko.- М. - 1983. 6. Lenindger, А. The fundamentals of biochemistry / А. Lenindger. - М., «Mir». - 1985. 7. Murry, R. Biochemistry of a man. / R. Мurry, D. Grenner, P. Meyes, V. Rodwell. - V. 1. - М.: Mir, 1993. - 384 p. 8. Murry, R. Biochemistry of a man. / R. Мurry, D. Grenner, P. Meyes, V. Rodwell. - V. 2. - М.: Mir, 1993. - 415 p. 9. Nikolayev, A.Y. Biological chemistry. / А.Y. Nikolayev. - М.: Medical information agency, 2004. - 566 p. 10. Fundamentals of Analytical Chemistry. / Ed. J.A. Zolotov. - Book 2. - M.: High School, 1996. – 461 p. 11. Reference book. Laboratory methods of investigation in clinic. / Edited by prof. V.V. Menshikov. - М. Medicine. - 1987. 12. Philippovich, Y.B. Fundamentals of biochemistry. / Y.B. Philippovich. - М.: High school, 1993. - 496 p. 13. Philippovich, Y.B. Exercises and tasks on biological chemistry. / Y.B. Philippovich, G.А. Sevastyanova, L.I. Schegoleva. - М.: Prosveschenie, 1986. - 144 p. 14. Philippovich, Y.B. Practicum on general biochemistry / Y.B. Philippovich and others.–Textbook. - М.: Prosveschenie, 1982. 15. ElliotV., ElliotD. Biochemistry and molecular biology. / V. Elliot, D. Elliot. - М. - 1999. Federal Agency of Education |
Последнее изменение этой страницы: 2019-06-19; Просмотров: 266; Нарушение авторского права страницы





 ceramide
ceramide  galactozilseramide
galactozilseramide